Tagged: oncology
The Art of War in Oncology
“Strategy without tactics is the slowest route to victory. Tactics without strategy is the noise before defeat.”
― Sun Tzu, The Art of War
So a bit of brainstorming / mind dump ahead of a lecture on Saturday.
Oncology has come a long way in the last two decades. Some cancers, even when metastatic, have become chronic diseases. In particular this is the case for beast, colon and prostate cancer, and in some selected cases even lung cancer. This raises some important considerations about how oncologists approach the treatment of cancer.
In the past a die was cast and essentially the patient chose to take the poison (chemo) or not and if they took it and it worked then fantastic, and if not, well that’s the way it was meant to be.
Now, for many cancers, there are multiple lines of therapy. There are options for intermittent and maintenance treatment. And the paradigms are changing. In the past ‘systemic diseases’ were not treated with locoregional therapies but now it may be appropriate. We are moving to an era where the combination of targeted therapies and selective surgical cytoreduction, regardless of cancer type, becomes the norm rather than a situation where the rules are being broken.
So for the oncologist we must start thinking strategically about the goals of treatment.
If the aims change from achieving tumour response or prolonging life to cure (in the case of metastatic colorectal cancer) or achieving 5 year survivals in the metastatic setting then fundamentally different strategies are needed. Specific tactics we might pursue are maximal cytoreduction whether by chemical or surgical means, maintenance therapy, toxicity reducing therapy, planned treatment interruptions, immunotherapy and other maneuvers. Thinking not just what will be first-line therapy will be but looking ahead to the long-term strategy is required. Do you hold some treatments in reserve?
It is also important to think about chronicity and the effect it has on the whole person. I find my patients are stunned when I run out of conventional treatment options an yet they remain well, apart from the toxicities already inflicted. In this case there must be a lot of preparation for the eventual physical but not psychological surrender. It must be understood that many battles will be fought and won but the overall war could be lost but it doesn’t constitute giving up.
It must also be remembered that strategy is created in the midst of conditions of uncertainty. This can be communicated but only addressed by making life as normal as possible.
In addition to setting
A turn of phrase in oncology
Communication in medicine and perhaps especially in cancer care rests on the interpretation of words.
Today I had to deal with the retort ‘but your colleague said that the chemotherapy I had was the best available for my cancer….so isn’t what you are offering me now not as good’.
So let’s strip this down. ‘The best available’ comes with caveats – the best available chemotherapy (just ignoring some of the new drugs) for melanoma has between 5 and 15% chance of shrinking deposits of melanoma. It is clear that ‘best available’ – at least in the eyes of the prescriber – is not the same as saying the treatment is effective for everybody. A treatment can be the best we have for all-comers but in reality the overall results can be pretty poor. The big problem is that most treatments don’t work for everybody: I can only get around this by saying that a treatment is the best option (compared to other options) and that even though a treatment is the ‘best’ for all-comers there is no way of predicting, for most drugs, which person will be the one who benefits.
Because of these vagaries we also need to be aware that just because one treatment didn’t work it doesn’t mean another might not – it may be that second treatment is better than the first – we just don’t currently have the means to predict which was the right treatment in the first place.
The trick for oncologists and other physicians – pick your words carefully – or take the time to explain what you mean.
Are the Hallmarks of Cancer a Good Framework for Teaching Oncology?
One of the challenges in teaching medicine and in particular sub-specialty medicine is the sheer volume of information to be digested. The commonest refrain I hear about studying the discipline of interest, in particular from new trainees in medical oncology, is ‘I don’t know where to start’.
There are many potential approaches.
There is the traditional basic science to clinical science approach. For example starting with the relevant biochemistry, anatomy, etc and building up towards practice.
There is the problem-based learning approach which is good for clinical scenarios but perhaps doesn’t encourage an understanding of depth.
Another approach applies templates to diseases. For example if we consider breast cancer one can think about the epidemiology, screening, prevention, adjuvant treatment and treatment of recurrent disease. The same template could be applied to each cancer type. There are common themes and also variations and differences between each cancer….but the basic themes are the same.
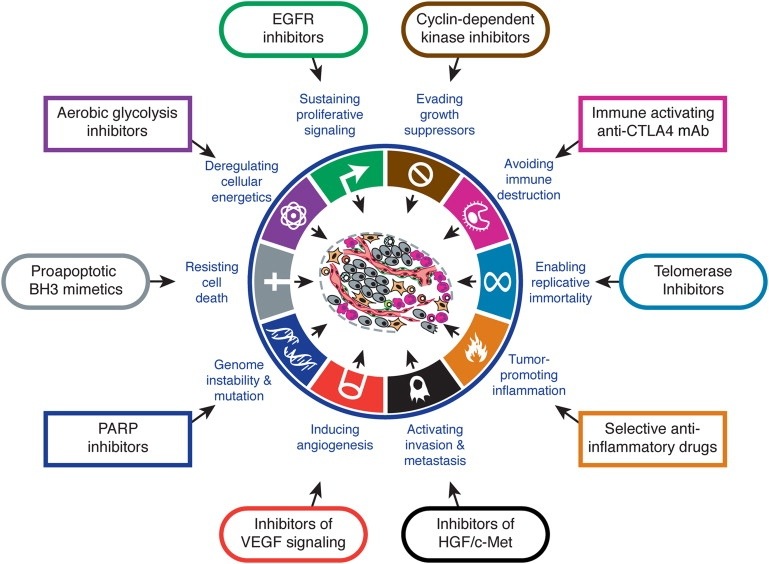
Arguably the latest approach is that of looking at the Hallmarks of Cancer as proposed by Hanahan and Weinberg in Cell (2000). The authors propose that there are key characteristics that cancers acquire that distinguish themselves from non-cancers. Although there are some criticisms that some of the hallmarks also apply to benign tumours, broadly speaking the concept provides a useful way for thinking about how cancers behave.
I think Hallmarks of Cancer is a useful framework for teaching oncology. What makes it useful if that you can think about high level concepts such as sustained angiogenesis or evasion of immunoregulation or self-sufficiency in growth signals or any of the hallmarks as having potential for application across the spectrum of oncologic interest: the hallmarks inform aetiology, diagnosis, prognostication, and potential treatment strategies. It provides a framework that facilitates both understanding complexity and engaging reductionism. It is the view from the plane that lets us know the concepts but enables closer examination.
Trainees need to familiarise themselves with The Hallmarks of Cancer and apply it to their studies.
Oncology versus palliative care
So I’ve just read this article in KevinMD about oncology and palliative care: The Tension Between Oncology and Palliative Care
Whilst I agree with the overall sentiment I think we can generally do better. First of all – this isn’t an issue unique to oncology – it is important for all sub-specialties and all patients/consumers where end-of-life is an issue.
Secondly this is a societal issue. Bottom-line is that nobody lives forever and so thinking about these things is important for both individuals and society. Society needs to get beyond the notion that technology trumps death.
Thirdly we need to move beyond palliative care as end-of-life care to the notion that supportive and symptomatic care is useful throughout the whole illness. This will both improve outcomes overall and prevent harm.
In an ideal world there is no oncology versus palliative care, there is just care.
