Category: Medical Education
Getting the specialist training job you want
When I was starting out in medical oncology my colleagues used to fret about there not being any jobs when we finished training. This wasn’t the case but it is starting to be true now. Although there are some early signs of exit block into consultant positions the emerging gap seems to be in advanced training positions. The reality seems to be that there are more potential trainees than jobs and this is starting to be a problem for all specialities. So if you want to progress from basic training to an advanced training position here are a few tips:
(1) Obviously pass the exams
(2) Treat every day as a job interview: you may not know who your future employers are
(3) Make your interests known but don’t be cocky or overbearing
(4) Do your due diligence – find out about the department you are interested in: talks to registrars already doing the job
(5) Pre-interview – meet your potential future supervisor
(6) Do something that makes you different from the rest of the pack: don’t just be somebody who has been to medical school and passed exams.
(7) Tell the interviewers about what makes you special
(8) Find out what types of question are asked at the interview and think of good responses
(9) At the interview always use personal anecdotes and experience in response to the questions
(10) Have a back up plan
Vocational training has a nomenclature problem
Physician trainees having just completed their viva examinations are anxiously awaiting results and are deciding they want to do for the rest of their lives: they are about to embark on what is called vocational training. This is supposedly training for which these individuals have a special calling – like the priesthood.
In reality many of my peers and my juniors seemed/seem to have no idea what they have a vocation for and in fact base their sub-specialty on a variety of factors including exposure (it was the best of a bad bunch), lifestyle choices (financial , overtime/shift-work), brains/brawn (physicians vs. surgeons), and even parental expectation. As a consequence I often see fully qualified professionals who are not suited for their ‘chosen vocation’ for a whole variety of reasons ranging from technical incompetence, through to boredom and burnout.
I ultimately went down two vocational training pathways: medical oncology and clinical pharmacology. Notably I had always thought my vocation was psychiatry. I did a consultation-liaison psychiatry term for my option term in a New York cancer hospital and loved it but when I returned to do a general psychiatry term it really didn’t gel – I didn’t hate it but at the time I thought it was (and perhaps remains) flawed both in philosophy and science.
As it happened I did 2 terms each in medical oncology, haematology and gastroenterology and a term in palliative care and thoroughly enjoyed them: so what to I do now? – gastrointestinal oncology. Oncology lead me to drug development and an interest in quality care and this in turn lead to clinical pharmacology as a second specialty.
I could tell you why I like these specialties but I can’t actually tell you why I ended up here rather than performing cardio thoracic surgery (although I do often tell patients I could take them apart I just couldn’t put them back together again).
Unfortunately many trainees don’t get broad enough exposure to different disciplines in order to find their calling. In addition their modes of practice often don’t reflect what it is like as an actual consultant. For example many doctors get put off oncology because of the death and dying aspects as they only do inpatient work and no outpatient work – this is not a unique problem.
What I can tell you is this: get exposed to as much as possible and then do what you really enjoy and have found satisfaction doing. The success, career-wise, will follow-on and hopefully you’ll never get bored. In medicine never view the practice of medicine as a view to making money: if you take this pathway you need to remember the only way to make money is volume (i.e. lots of work). You’ll make more than enough doing what you really like and perhaps more than you expect. But if you really view financial gain as the reason for your ‘vocation’ then you chose wrong.
Finally don’t view a ‘vocation’ as being a singularity. First and foremost physician sub-specialty trainees need to remember that being a physician brings skills and opportunities to do things in the same way that law or commerce does.
Advice for registrar job interviews
So it is ‘pre-interview’ season…the time when basic physician trainees who have done their Part 1 exam come looking for advanced training positions. Finally somebody asked me what to do at the interview. So in the interest of equal opportunity here are my tips:
(1) Fill out the application form correctly. Spelling errors show a lack of attention to detail.
(2) Nominate recent referees and let them know or ask their permission for the nomination. Not having recent referees suggests that there might have been a problem. Ideally nominate somebody in the specialty you are applying for.
(3) Actually know what the job description is and if you are applying for a specific organization know what is special about that organization.
(4) Make yourself different to the other candidates: set yourself apart. Most registrars have similar levels of experience and training so the interviewers want to know what makes you different from the others. Everybody has passed the exam and has a suit. And, note to candidates…..absolutely every interviewee for the last 20 years has sent …”this is a really exciting time in oncology with lots of new treatments and opportunities for research”. It’s time to come up with something different.
(5) Ask the interviewers to repeat the question if you didn’t get it the first time: this will give you time to think.
(6) Use examples from your own experience: the interviewers want to know how you specifically deal with problems and being able to use your own experience makes it more than hypothetical.
(7) Find an opportunity to talk about your special skills. It doesn’t matter what they are. Let’s say in your spare time you are a concert pianist……this shows dedication and application… the interviewers have learned some important information even though it doesn’t appear to relate to doctoring.
(8) Think about the likely questions: almost every job interview on the planet has questions about dealing with conflict, team-work, dealing with stress, time-management, etc. Think of examples ahead of time.
(9) Many interviews also ask about strengths and weaknesses…..so think about this ahead of time and when you answer these questions relate them to the position description.
(10) Have an answer if the interviewers ask ‘where do you see yourself in 10 years time?’. If you don’t know then be honest about it.
(11) Asking questions at the end is fine and enncouraged.
Whilst these tips are aimed at oncology registrars they apply across all specialities and many other jobs.
Effectiveness versus Efficiency in the Medical Consultation
One of the challenges in training registrars is trying to get over the apparent emphasis on the speed of consultation, or what you might call – churn. For doctors in clinical and rooms there is a set amount of time and a certain number of patients. You could argue that there might be more patients than a reasonable amount of time and yes one could take the approach that one will take as long as necessary to o deal with all the patient issues but reality dictates that if you take that approach you probably won’t actually see al that many people and the population might be less-well served as a result.
Bosses can get grumpy with their registrars is they only see a few patients in their clinic and the clinic runs over time. Equally so the registrars might feel they are taking too long or perhaps not being thorough enough.
Rule 1 should be that every consultation isn’t a so-called long-case. I like to say…if there is nothing wrong then there is not much to say. Rule 2 should be that the focus is on effectiveness not efficiency. By this I mean – did you identify and sort out the problem? You can still this in a timely manner – you just need to adjust the pace to the circumstances. In my experience patients don’t like to be rushed but on the other hand they are more concerned with having their issues addressed and if you can do this the time it takes is of lesser importance. Flowing on from this then Rule 3 must be ‘deal with the most important concern to the patient’ – this is perhaps the hardest part. For starters what the doctor thinks is important and what the patient thinks is important isn’t always the same. Secondly what the patient thinks is important isn’t always transparent….this is the ‘there’s one more thing doc’ discussion.
So in summary – work out what’s important and deal with it and move on. This is effective and efficient consulting for a resource poor reality. In other words, until we get more resources to support whole person care and the time-unlimited consultation ‘Don’t sweat on the small stuff’
Are the Hallmarks of Cancer a Good Framework for Teaching Oncology?
One of the challenges in teaching medicine and in particular sub-specialty medicine is the sheer volume of information to be digested. The commonest refrain I hear about studying the discipline of interest, in particular from new trainees in medical oncology, is ‘I don’t know where to start’.
There are many potential approaches.
There is the traditional basic science to clinical science approach. For example starting with the relevant biochemistry, anatomy, etc and building up towards practice.
There is the problem-based learning approach which is good for clinical scenarios but perhaps doesn’t encourage an understanding of depth.
Another approach applies templates to diseases. For example if we consider breast cancer one can think about the epidemiology, screening, prevention, adjuvant treatment and treatment of recurrent disease. The same template could be applied to each cancer type. There are common themes and also variations and differences between each cancer….but the basic themes are the same.
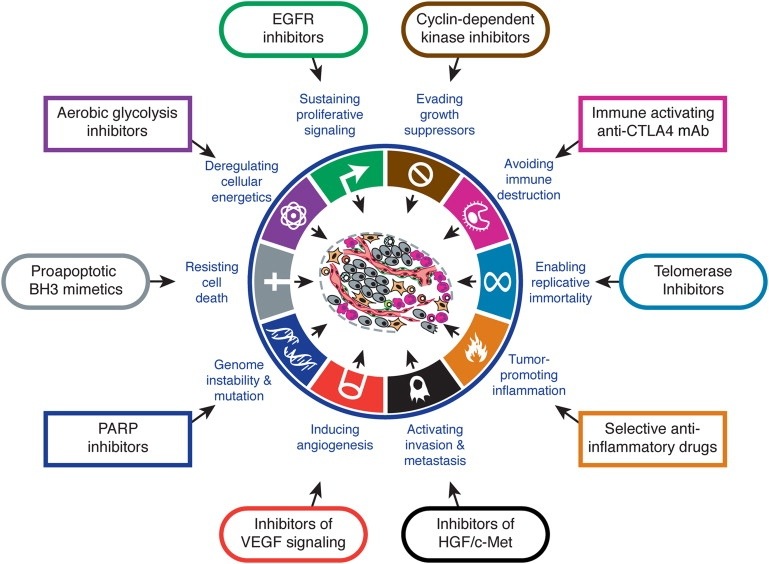
Arguably the latest approach is that of looking at the Hallmarks of Cancer as proposed by Hanahan and Weinberg in Cell (2000). The authors propose that there are key characteristics that cancers acquire that distinguish themselves from non-cancers. Although there are some criticisms that some of the hallmarks also apply to benign tumours, broadly speaking the concept provides a useful way for thinking about how cancers behave.
I think Hallmarks of Cancer is a useful framework for teaching oncology. What makes it useful if that you can think about high level concepts such as sustained angiogenesis or evasion of immunoregulation or self-sufficiency in growth signals or any of the hallmarks as having potential for application across the spectrum of oncologic interest: the hallmarks inform aetiology, diagnosis, prognostication, and potential treatment strategies. It provides a framework that facilitates both understanding complexity and engaging reductionism. It is the view from the plane that lets us know the concepts but enables closer examination.
Trainees need to familiarise themselves with The Hallmarks of Cancer and apply it to their studies.