Tagged: medicine
Things they didn’t teach in medical school: Part 26 – Giving fitness advice
Yesterday I wrote how medical school doesn’t teach much about giving dietary advice. Well the yin to diet’s yang is fitness and exercise. This is also a commonly asked question – what exercise can I do? Is it OK to exercise? Well this is important for both the sick and the well….and I’ll make a confession – I’m not one for formally exercising although my fitbit tells me that generally I do more than 10,000 steps a day.
In some cases it isn’t good to be physically active or to undertake certain exercises like heavy lifting – for example, if you’ve just had abdominal surgery you might increase your risk of hernia. Certain types of exercise – like heavy impact contact sports might be dangerous for a person with bone metastases. But in general keeping active, if not actually exercising is important.
After a stay in hospital many individuals are deconditioned. This happens very quickly with any bed rest – just like an athlete in the off-season. In this case getting back to exercise is very important for return to normal quality of life. There are simple things to do: use a chair for support to stand up between commercial breaks on television, climb back and forth along a small flight of stairs (with a railing) and take progressively longer walks around the neighbourhood (checking out their mail boxes).
Increasing exercise and fitness levels may be important in very specific conditions such as rehabilitation after heart attack or heart surgery, patients with chronic airways disease or after cancer. Increased activity after cancer may actually reduce risk of relapse and prolong life expectancy – the trials are ongoing. Frail and elderly patients may benefit from exercise to reduce falls.
The other aspect of exercise is how to do it. Recent evidence suggests that prolonged periods of exercise are not necessarily the best way of achieving fitness (and weight loss). Interval training with short bursts of intense activity may be more effective. Mixing up different types of exercise might be important for achieving different aims.
Doctors and future doctors need training in giving advice on fitness and exercise.
Things they didn’t teach in medical school: Part 25 Giving dietary advice
One of the commonest questions my patients have is “What should I be eating?”
Interestingly, I don’t think I was taught very much about basic nutrition at medical school. We did learn about the deficiencies such as scurvy (vitamin C) and beri beri (thiamine) but I don’t think we were taught much about normal nutrition. We definitely weren’t taught anything about nutrition in sickness or aberrant nutritional status. This is somewhat unfortunate as most of my patients are either malnourished as a consequence of their cancer or the treatments for their cancer. Living in modern society, most of the remaining people I see are overweight.
Now, you could argue, as the Nutrition Science Initiative does, that we don’t actually know what the ‘correct’ diet is and that most of what has been taught or is understood is wrong, or flawed, but I guess you have to start somewhere. Currently the debate is raging around whether the culprit for obesity is fat, carbohydrates or sugars, or lack of exercise. Various diets – vegan, paleo, Atkins, Mediterranean, etc – argue over the proportions of fat, sugar, carbohydrates, sugars and proteins allowed in the diet. Regardless of the best proportions the fact is that if doctors asked their patients they would soon discover that many wouldn’t know which foods contained what.
Future (and current) doctors need to be taught the best available information about dietary composition and also the behavioural techniques that have been demonstrated to assist in weight loss (or gain). Doctors also need to know how to manage the malnourished patient. Now we can turn to dietitians and nutritionists for advice this is knowledge is so intrinsic to healthcare that it should be considered essential learning. And besides….we might improve the hospital food.
Things they didn’t teach in medical school: Part 23 Saying goodbye to patients
One of the things I haven’t quite got the knack of is saying goodbye to patients. I’ve recently looked after two young women the same age as myself. Both with children similar ages
In my job as an oncologist I often establish long-term relationships with patients. These relationships can span years and involve periods of fortnightly visits, stays in hospitals, and the roller-coaster ride of good and bad news. Some of these patients genuinely considered to be friends.
Unfortunately, as is the case for cancer and a lot of other diseases, the inevitable end comes. With years of experience doctors becoming increasingly good at predicting the time to end-of-life. The reality is that I know that sometimes when I am consulting with a patient, either in the rooms or on a ward, it will be the last time I see them alive or in some cases the last time I will be able to talk to them. In some cases I know they are going to hospice and won’t return.
I’m sure that the patients often know as well but nonetheless we do the dance, “I’ll see you tomorrow” or “make an appointment for two weeks”. It is an opportunity for imparting hope but a lost opportunity for saying goodbye.
In Annals of Internal Medicine (2005: 148(8), p. 682) Anthony Back offers a list of tips around saying goodbye:
(1) Choose an apropriate time and place
(2) Acknowledge the end of routine contact and the uncertainty about future contact
(3) Invite a response and use it as data about the patient’s state of mind
(4) Frame as an appreciation
(5) Give space for the patient to reciprocate and respond empathetically to the patient’s emotion
(6) Articulate ongoing commitment to care
Like most of these communication experiences it is important to practise and to remember to remember that communication is jazz – you will have to improvise.
Things they didn’t teach in medical school: Part 22 Project Management #TEDMED
Something not taught in medical school is project management. Although at medical school you might undertake assignments and similar activities, unless you are allocated a research project it is unlikely you will have any formal instruction in project management. I, in fact, don’t consider myself to be especially good at hands-on project management and work better as a collaborator on projects rather than running them directly. Project management is related to time management. You an think of time management as about managing your time to do projects and visa versa project management is a about completing tasks on time.
It is important first of all to recognise a project when it is either handed to you or you come up with the idea.
For me the simplest definition of a project is any activity that can be broken down into smaller tasks to produce an outcome which is more than the sum of the individual parts. Using this definition a project may be small e.g. preparing the meeting roster for a year or large e.g. designing a new medical school curriculum.
There are some tips for managing a project:
– really identify what the purpose and aim of the project is and visualise how the finished project will look – what are the deliverables
– estimate the resources you will need and the time you will need
– identify who is critical to your project – for example, if you need statistics advice for a research project get it early
– break the project down into the smallest tasks possible and work out what in what order they should be completed (and which tasks depend on another tasks being completed – a dependency)
– identify what will stop the project from being finished
– based on the above decide if your project is feasible or not
– identify stakeholders and collaborators
– once the project has started have a regular review process to check progress
Last night at the opening session of TEDMED 2013 Professor Rafael Yuste spoke about the relationship between pursuing big science and his passion for mountaineering. He broke them both down to 3 steps: assemble the team, map the course and keep the summit in sight. The scientific summit he plans to climb is the Brain Activity Map now known as the Brain Inititiative which was announced by Barack Obama 2 weeks ago. This is the moon project or human genome project of the decade. You can see him talk @TEDMED
Things they didn’t teach in medical school: Part 21 – you can do more than look after patients
So I don’t really like the title I came up with, after all, looking after patients is pretty important. What the title refers to is the observation that medical training equips you for more than medical practice – although nobody teaches you that.
I haven’t quite reached the point of abandoning face-to-face patient care but increasingly I spend my time undertaking activities that might be considered influencing care rather than undertaking care.
It is often observed that many people with law degrees don’t end up being day-to-day lawyers. Well this probably applies to a lot of the core professions. Last week I ran into a basic scientist who now has a job as a research strategist and commercialisation advisor.
So what is the common theme?
Professional training really consists of two themes. One is largely around the technical knowledge relevant to the discipline – i.e. the law for lawyers, economics for economists, anatomy/physiology/pharmacology for doctors, etc, etc. The second is around problem solving. Professionals/experts fundamentally have the job of correctly identifying problems and questions and then trying to solve them. In medicine my job is to ‘diagnose’ the patient’s illness, prioritise the management problems and solve them.
Now, as I sit on hospital administrative committees and company boards, my job is the same. Identify the problem and find the solution.
This week an end came to an advisory committee that I have sat on for the last 6-7 years. The advice was around eHealth and electronic decision support. Whilst I do have some understanding and technical knowledge of these areas my real contribution to the group was to look at problems from a different perspective, to re-define the problems, to re-calibrate the discussions. This was also the role of my fellow committee members who were often drawn from different professions or different versions of my profession.
Some of my colleagues and peers make a complete jump and leave day-to-day medicine altogether to pursue apparently different careers. I’m pretty sure they are out there diagnosing problems and finding solutions.
Not a good week for the Therapeutic Goods Administration and QUM
The Therapeutic Goods Administration (TGA) is charged with ensuring Australians can have confidence that the medicines and devices and other therapeutic goods that are sold in Australia and safe, effective and manufactured well. At a high level the role of the TGA is to practice evidence based medicine (EBM) and quality use of medicines (QUM). The last fortnight has seen poor outcomes on all fronts and both in the area of conventional and complementary medicines regulation.
In the first case a TGA proposed ban on combination products containing detropropoxyphene (DPP) was overturned by the Administrative Affairs Tribunal. DPP has been associated with death due to cardiac toxicity, albeit often in the situation of overdose. It is not considered to be a superior analgesic to common alternatives. Internationally the drug has been withdrawn from a number of jurisdictions because of safety concerns and available alternatives.
In the second case the vitamins giant Swisse has bypassed a ruling of the TGA that its’ diet pill does not have evidence to support its’ claims and has renamed the product and re-worded the claim. The product itself is the same. The registering process provides not oversight of this process and it can only be addressed through appeal.
Regardless of its’ best intentions in these cases the TGA seems hamstrung by the Act under which it operates. This is too the detriment of the general public and not in the spirit of the National Medicines Policy. In one case there is increased risk of harm without added therapeutic benefit, in the other little evidence of benefit. What is needed it not necessarily more onerous regulation but more thoughtful regulation and also education of the public, particular around complementary medicines.
These comments reflect my own personal opinion and not those of NPS Medicinewise.
Things they didn’t teach in medical school: Part 20 How to do meetings
So over the weekend I speed read Sheryl Sandberg’s book Lean In.
I was motivated by the useful summary by the NY Times David Brooks: “Think about Sheryl Sandberg’s recent book, “Lean In.” Put aside the debate about the challenges facing women in society. Focus on the tasks she describes as being important for anybody who wants to rise in this economy: the ability to be assertive in a meeting; to disagree pleasantly; to know when to interrupt and when not to; to understand the flow of discussion and how to change people’s minds; to attract mentors; to understand situations; to discern what can change and what can’t”.
This reminded me about something that is increasingly important in my life – going to meetings. In fact my colleagues give me a hard time because I’m a bit of a meeting junkie but this is only because they spend 4-5 hours a week in meetings as opposed to my 20.
If as a doctor you work in a hospital and you are engaged with the running of the place you will need to spend a lot of time in meetings. These range from meetings of 2-3 people to 20 or more. The reasons for the meetings will be diverse and they encompass education, environmental scanning (FYI meetings), working meetings (i.e. you are making decisions) and advisory meetings (where you are helping others make decisions).
There is a lot written about how to run effective meetings so I won’t re-iterate all of these writings. I will say however that you need to know what the purpose of the meeting is and at the end of any meeting there needs to be an outcome…a decision or an action arising. Bad meetings are staccato and without resolution whereas good meetings have ‘flow’ and resolutions. Meetings work when everybody who wants a say gets a say, diversity of opinion is expressed and the outcomes are determined by consensus (this doesn’t actually mean everybody likes the outcome but everybody agrees).
Overall David Brooks’ summary offers a nice approach to meetings.
One final thing you do need to know about meetings is when to say no….my rule is that unless it is exceptional there is no role for ‘routine’ meetings that happen only twice a year….almost by definition these don’t achieve anything.
There is a whole additional art to chairing a meeting – one which I’m just coming to grips with – and which will form another post.
Things they didn’t teach in medical school: Part 9B Self-management – or perhaps self-assessment
So perhaps this should have been part 20.
Assessing one’s own performance as a doctor is not taught at medical school.
The problem is of course that as a doctor there is a touch of the ‘God’-complex, not to mention a historical lack of scrutiny.
But on a more personal note it is actually very difficult to step-aside and assess your own performance objectively.
One way to do this is to focus on how you handled the difficult case. But in reality the difficult case was probably going to be difficult regardless of how brilliant a clinician you are and in many circumstances the reasons why the case is difficult is out of your control.
I think the real challenge is assessing overall performance. A little like assessing organisations you can assess processes and outcomes. Outcomes are the difficult measure because you don’t necessarily know how your peers perform and different doctors treat patients with different ‘degrees of difficulty’.
For both process and outcomes you can assess against benchmarks and guidelines but there will always be uncertainty about how these are set.
Finally one needs to have a personal reference point: do you aim for a consistent standard within a specific set of skills or do you have a reference of achieving both this, combined with progressive improvement & expansion of your skill-set.
I think the latter is the most important issue that needs to be addressed before the profession can embrace personal self-assessment. Do the practitioners know what their goals are? Do you graduate and coast or graduate and grow? Self-assessment needs concrete actions otherwise others will do it for us and no doubt in a way that won’t be helpful.
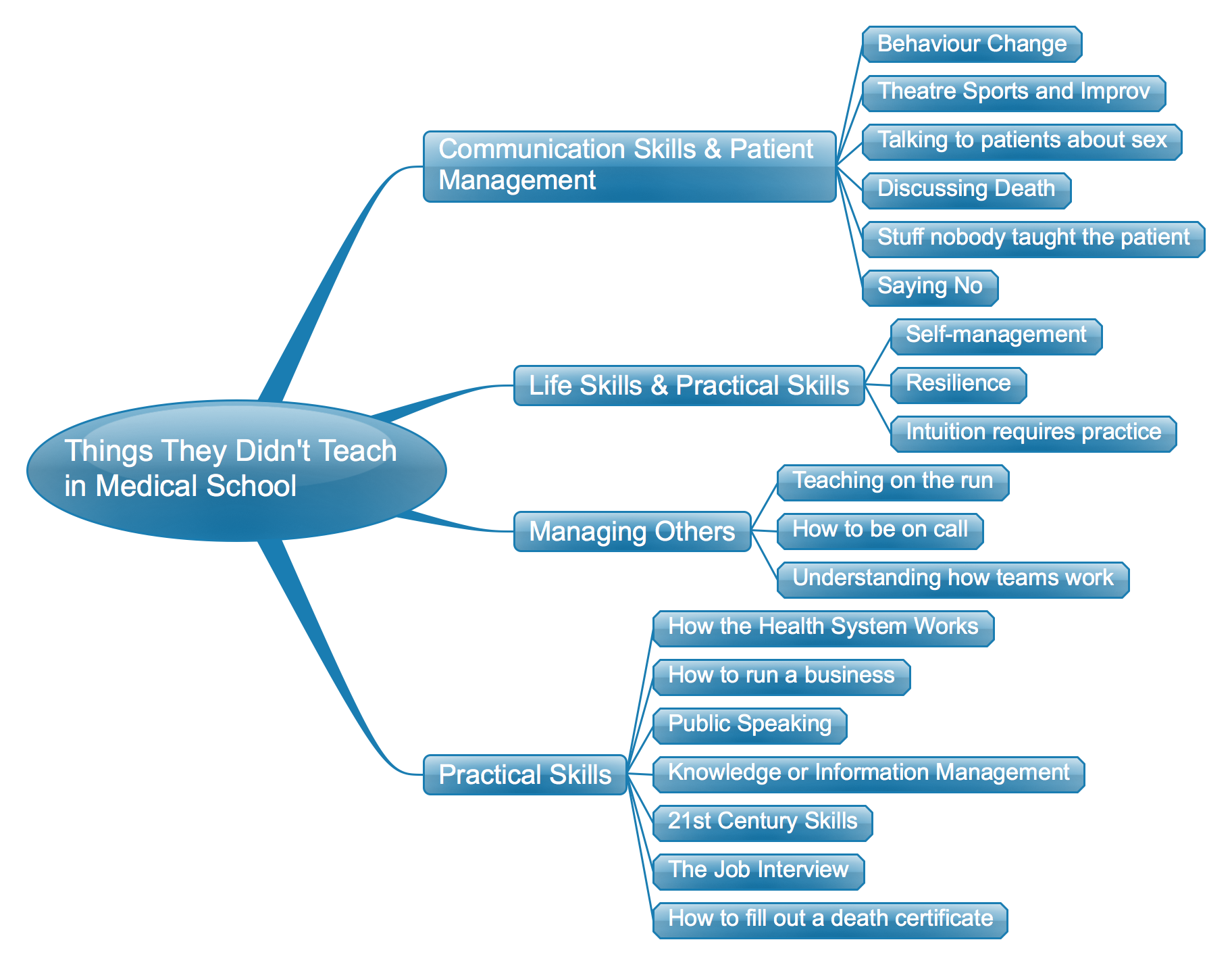
Things They Didn’t Teach in Medical School: The list so far – a mind map
Things they didn’t teach in medical school: Part 18 Intuition Requires Practice
The dogma of modern medicine is that it should be evidence based. Well this is true but in actual day-to-day practice the evidence is often only marginally helpful.
In actual fact we practice a lot of medicine based on gut instinct. And this gut instinct is learned from doing the same thing over and over again, by seeing similar cases and recognising what the outcomes will be. This is a type of evidence based medicine which we might call experience based medicine.
Let’s tale the example of dose-adjusting chemotherapy. There are guidelines about what to do but when you take a phone call you invariably don’t look up a guideline. I adjust the doses partially based on guidelines and mostly based on my experience of what will happen with dose adjustments. The reality is that practice makes, if not perfect, at least better.
