Tagged: medicine
Are the Hallmarks of Cancer a Good Framework for Teaching Oncology?
One of the challenges in teaching medicine and in particular sub-specialty medicine is the sheer volume of information to be digested. The commonest refrain I hear about studying the discipline of interest, in particular from new trainees in medical oncology, is ‘I don’t know where to start’.
There are many potential approaches.
There is the traditional basic science to clinical science approach. For example starting with the relevant biochemistry, anatomy, etc and building up towards practice.
There is the problem-based learning approach which is good for clinical scenarios but perhaps doesn’t encourage an understanding of depth.
Another approach applies templates to diseases. For example if we consider breast cancer one can think about the epidemiology, screening, prevention, adjuvant treatment and treatment of recurrent disease. The same template could be applied to each cancer type. There are common themes and also variations and differences between each cancer….but the basic themes are the same.
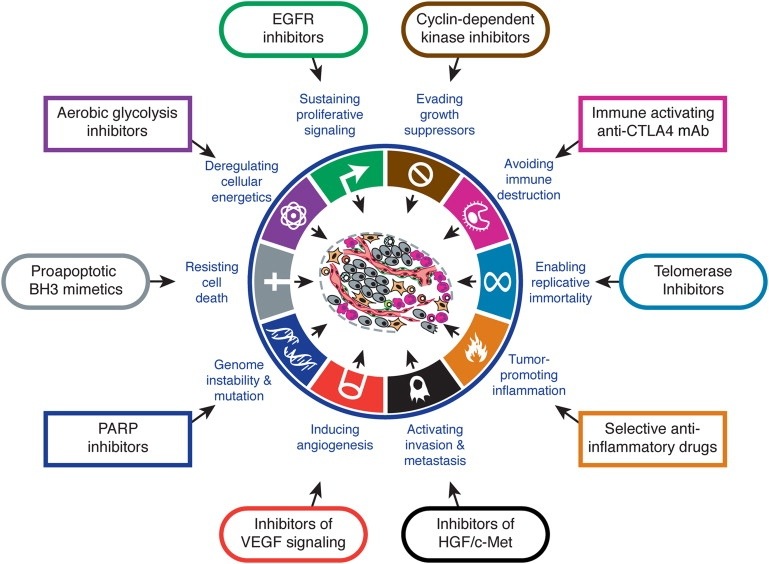
Arguably the latest approach is that of looking at the Hallmarks of Cancer as proposed by Hanahan and Weinberg in Cell (2000). The authors propose that there are key characteristics that cancers acquire that distinguish themselves from non-cancers. Although there are some criticisms that some of the hallmarks also apply to benign tumours, broadly speaking the concept provides a useful way for thinking about how cancers behave.
I think Hallmarks of Cancer is a useful framework for teaching oncology. What makes it useful if that you can think about high level concepts such as sustained angiogenesis or evasion of immunoregulation or self-sufficiency in growth signals or any of the hallmarks as having potential for application across the spectrum of oncologic interest: the hallmarks inform aetiology, diagnosis, prognostication, and potential treatment strategies. It provides a framework that facilitates both understanding complexity and engaging reductionism. It is the view from the plane that lets us know the concepts but enables closer examination.
Trainees need to familiarise themselves with The Hallmarks of Cancer and apply it to their studies.
Negotiating the religious obstacle course in end-of-life care and cancer care
As an upfront disclaimer I’ll note that I am an atheist.
Now that’s out of the way I’d like to think/write out loud about the problem of religion and spirituality in the care of cancer patients.
The role of religion in the overall outcome of cancer patients has been the subject of a lot of research and overall I’d have to say that the results are conflicting or inconclusive. There is no real evidence of improved outcomes with respect to the gold-standard – survival and/or cure. Spirituality and religiosity has however been associated with improved quality of life. There is mixed evidence, and this reflects my own experience, that religious individuals might choose less aggressive or more aggressive treatment at the end-of-life.
This makes it challenging for the clinician wanting to exploit religiosity for therapeutic ends. In some cases the religious person is sometimes reliant on their God for a miracle and to that end won’t accept a palliative pathway whereas in other cases the individual uses their faith as a crutch to help them deal with their impending death. Personally I feel that the latter pathway is the correct pathway from a theological perspective. My personal view is that many religious people don’t understand their religion (but again I’ll invoke my disclaimer at this point).
So what should the clinician do when it comes to intercalating a spiritual discussion into end-of-life care? The existing evidence suggests that access to spiritual care and support from spiritual care is low and also not provided by conventional medical systems. Yet it may play a role in helping individuals clarify their wishes. Should I as a clinician try to exploit spirituality to steer a patient to a conservative path of care? Alternately should I ask for a ‘religion consult’ in the same way that I might ask for a ‘cardiology consult’?
At the end of the day, and until there is more evidence, I think the clinician needs to tailor these discussions based on their gut instinct but I tell you now, it takes a lot of practice.
Things they didn’t teach in medical school: Part 33 Looking after colleagues and their families
Oncology can be a tough specialty with difficult emotional demands. These demands are compounded when you are called on to look after colleagues and/or their families. My earliest encounter with this was actually as a resident medical officer. I remember doing an evening shift and the nurses asking me to see the Professor of Surgery who had just been diagnosed with cancer and was due for a colonoscopy – the nurses were concerned that he had been drinking his bowel prep but hadn’t yet opened his bowels….I assured them he would. Later as a junior registrar I would accompany my bosses to see consultants who were hospitalised – this was just incorporated as a matter of fact into ward rounds.
Now I’ve moved up the food chain and am a boss myself I am called upon to look after the family of colleagues and no doubt I might have to treat colleagues for diseases in my specialty (rather than just their day to day ailments). The hardest thing I’ve had to do in this space is look after a family member of somebody who had been both a mentor and a work colleague. I’ve also had my own family members looked after by colleagues and whilst I’ve not necessarily agreed with the treatment pathways I’ve recognised that this is not my doctor-patient relationship to negotiate.
There is no doubt that you treat these patients differently. I don’t think this is actually providing better care or different for the patient themselves but you might make the extra phone call and provide more regular updates.
I think there are two key practice points to providing this care:
(1) actually, as much as possible, do not do anything different to your usual practice &
(2) remember, as always, to treat the patient, not the family (obviously whilst still engaging with them).
If you are a doctor with a family member being looked after by another doctor then there is a bit of quid pro quo…..don’t second guess your colleague and give them advice what to do – you trusted them enough to look after your family member in the first place.
Things they didn’t teach in medical school: Part 32 Coping with repetition, dealing with boredom
Medicine is an occupation that can provide enormously satisfying intellectual and creative challenges. But like any job where there are repetitive tasks it can have it’s boring moments. Becoming a specialist requires that one become expert through constant practice and repetition yet once mastery is achieved the continued day to day repetition can start to be frustrating. You might find yourself having the same conversations over again or performing tasks on auto-pilot. The problem with this is it can lead to laziness and mistakes, especially if boredom is combined with tiredness or is a symptom of burnout.
There are different ways to combat boredom. One of the reasons people get bored is a lack of challenges. I always know that my trainees are happy to become consultants and not to general overtime because they will no longer get called to see ‘chest pain’, well at least not as regularly. They’ve reached the point where this diagnostic task is no longer interesting – they need new challenges. So creating new challenges is a way of getting out of a rut. This might take the form of trying to improve your own performance – the perfectionist approach.
Another way to alleviate the boredom is the theme and variations approach. By this approach you do something routine in a different way…this can be just mixing up the way you explain something or you can consider it an experiment to find the best way.
The obvious way to deal with the non-creative tasks is to create opportunities for creativity. I’ll call this the portfolio approach. Many clinicians I know regard their clinical jobs as their bread and butter and they get broader satisfaction from their other roles such as researcher, teacher or even administrator. These other roles act as distractors and relief from the day job.
There are, of course, other ways, to deal with the boredom – regular breaks and holidays, learning new skills, and getting your work life balance right….and of course looking out for the next interesting patient problem to give you that ‘why I got into this in the first place’ feeling.
PS. my joke to my inpatients is that the commonest reason people die in hospital is boredom….don’t let boredom kill your career
Oncology versus palliative care
So I’ve just read this article in KevinMD about oncology and palliative care: The Tension Between Oncology and Palliative Care
Whilst I agree with the overall sentiment I think we can generally do better. First of all – this isn’t an issue unique to oncology – it is important for all sub-specialties and all patients/consumers where end-of-life is an issue.
Secondly this is a societal issue. Bottom-line is that nobody lives forever and so thinking about these things is important for both individuals and society. Society needs to get beyond the notion that technology trumps death.
Thirdly we need to move beyond palliative care as end-of-life care to the notion that supportive and symptomatic care is useful throughout the whole illness. This will both improve outcomes overall and prevent harm.
In an ideal world there is no oncology versus palliative care, there is just care.
Things they didn’t teach in medical school: Part 30 Continuing the conversation after the consultation
One of the things they didn’t teach in medical school is how to continue to the conversation of the consultation after the actual physical consultation is over. Supposedly shared decision making leads to better decision satisfaction and outcomes but what happens once the patient leave the consulting room.
In some cases they leave with a pile of printed information. They may have taken their own notes. Or a carer may have taken the notes and been the second pair of ears. But I know the wrong messages may have been taken away or there will be lots of questions.
One way to deal with the problem is to ensure that the patients have had an opportunity to ask the questions in the first place – question prompt lists can help with this.
Another potential way is to provide a record of the consultation. This can be a written summary or alternately it can be an audio record of the consult. Some doctors are set up to do this but these days it most commonly happens when patients ask me if they can record the conversation and then they use their mobile phone.
An alternate potentially useful method is to develop your own resources to refer the patients to. I’ve just started, albeit extraordinarily slowly due to time commitments, to develop videos using the Explain Everything platform. Hopefully my patients will find these useful both for innformation about their treatment and to inform decisions.
Here is my talk on Xeloda Side Effects
Repurposing old and unsuccessful medications
Sometimes drugs are tested in clinical trials and don’t meet their goals. In many situations this is the end of development for these drugs. Notably, given the amount of science that has gone into development of many agents it is not inconceivable that they could be repurposed to treat difference problems. Sildenafil (Viagra) is a case in point – it started as a treatment for hypertension and ended up being used for erectile dysfunction. This was a chance development and in reality most companies aren’t interested in pursuing further trials in other conditions given the cost of drug development.
In some circumstances there is a superimposed ethical problem. Some trials are stopped for overall lack of benefit but some participants may well have benefited. This often happens for orphan indications. This is actually probably true for most medications – they only work in some of the people that take them, in much the same way that they only cause adverse effects in some of the people that take them. The case of arbaclofen for treating Fragile X syndrome and autism is a recent example http://www.nytimes.com/2013/06/07/business/an-experimental-drugs-bitter-end.html?smid=pl-share
There are however potential ways to overcome the problem of withdrawing a ‘possibly effective therapy’. Regulators are now partnering with industry to deliberately encourage research into discarded medications. Medications which incidentally have been shown to be safe through previous clinical research but ineffective in their original target research. The NIH funds such a program http://www.ncats.nih.gov/research/reengineering/rescue-repurpose/therapeutic-uses/therapeutic-uses.html
A potential pathway in the case of arbaclofen to continue studies in these patients, and also supply of drug, would be crowdsourcing. The owner of the intellectual property – having decided that the product is worthless – could agree to either write-down its’ ownership and make the IP public domain or alternately allow public development with minimal claim on any patent royalties if the product is successfully developed or alternately to retroactively cover costs of development undertaken in the public domain through a limited buy-back of rights – all of these approached would be significantly less expensive than the traditional methods of developing the drug and financing that development. The drug manufacture could no doubt be cheaply outsourced to an Indian manufacturer and study data collection could move to open source models with independent review.
Developing novel methods to pursue drug development both of old and new drugs is important to ensure new treatments are developed and to ensure to viability of an industry which is increasingly poor at developing successful new drugs and increasingly unlikely to have them paid for by cash-strapped healthcare systems.
The business model and bioethics of the anti-aging drug development
In the last month I’ve been to @TEDMED and seen Laura Deming talk about prolonging life. I’ve also been to #TEDxSydney and seen David Sinclair discuss his research in anti-aging drug development. Each week there seem to be new publications in the scientific journals and reaching the mainstream media. There has been success in animals and human trials are in progress.
I don’t need to tell you how obsessed the world is with aging and slowing it down. Even if we get past the issue of vanity the key metric of economic prosperity is probably not per capita GDP but the life expectancy of its’ citizens.
Let me propose that an actual treatment, and I assume it ill be a drug, that slows aging, will be a game changer for how the pharmaceutical industry functions.
If we look at the history of prolonging life expectancy we can really identify a few key transition points that include:
– basic sanitation and food and water security are probably the single most important things for prolonging life. Keeping clean and having regular access to safe food and drink is the starting point. Value adds include refrigeration, electricity (to support heating and cooling) and running potable water). The main impact of these ‘innovations’ is to reduce infectious disease.
– second order innovations include vaccination and antibiotics to fight infectious disease
– the third tier of innovations is prevention and treatment of diseases related to abundance i.e. heart disease, tobacco related illness and although it hasn’t been properly tackled yet, morbidity related to obesity.
I like to say to my patients that they didn’t die from infectious disease in childhood and their heart specialist kept them alive after their heart attack so they can live long enough to get cancer or dementia (or death from complications of frailty). Successful anti-aging drugs will need to not only prolong life but reduce the chances, or at least, not increase the chances of cancer or dementia, and do so in the context that the chronologically aging but not physically aging person is staying fully functional. This is a very important distinction: often doctors will refer to a ‘good 85 year-old’ versus the ‘poor 75 year-old’ as a reference to physiological age not chronological age.
So lets assume this ideal anti-aging drug can be developed and lets assume it is actually very successful i.e. it prolongs functional life in good health by a meaningful period of time….let’s say a decade. What does it mean for the pharmaceutical industry?
Well I think we need to look back at the other game changers in longevity promotion listed above. Access to food, water and sanitation is considered a basic human right. The second and third levels of innovation probably haven’t quite become universal human rights but only in the sense that they are contingent on the first innovation and the reality is that those without access to the 2nd and 3rd set of innovations often haven’t had their universal human rights fulfilled.
So I would make the case that should an anti-aging drug become available, and if it demonstrates tangible flow on health (an other benefits) then access to the drug will become a right rather than a privilege based on economic advantage. In this case there might not be the usual monopoly advantage that pharmaceutical giants usually exert as populations won’t accept it. And remember, it is more than likely the drugs will need to be taken forever, from what ever age is deemed acceptable.
Now it could play out that the usual pathway of drug access occurs and that actually by the time we are really understanding the pros- and cons- of these agents the patents are expiring but I don’t think this is really going to happen. These drugs, if they really meet the aims of prolonging life without complications, will be marketed like Viagra-on-steroids.
Clean water is a universal human right. Who would have thought that internet access would become a universal right but it is rapidly becoming so. A successful anti-aging medication would probably also become a universal right.
Addendum: people will argue we shouldn’t use such drugs because it isn’t how things are meant to be (i.e. we have a natural lifespan). We maybe so but this quite simply isn’t what humans do….we meddle with nature to try and make it (and ourselves) better…..there may be a philosophical argument but it will be trumped by reality.
Realizing different perspectives to identify the value proposition for whole person care
Disclaimer: thought bubble alert – this is a bit of thinking out aloud as I work through some ideas about personalised care versus systemic change in health care. So here it goes.
Whole person care is elusive both in definition and implementation.
The definition of whole person care articulated by Hutchinson focuses on the distinction between the healthcare worker being focused on ‘curing’ the patient and ‘healing’ the patient. Yet this is only one of many attempts to address the progressive depersonalisation of medicine and healthcare. When I trained these problems were discussed in relationship to the biopsychosocial model of healthcare. Patient-centred care is probably the official term for a more personalised approach to medicine despite the parallel development of the whole person care movement. Another group refers to integrated models of care. No doubt the advocates for each of these models of care draw distinctions between their definitions and goals, and also different parties (patients, nurses, physicians, and healthcare systems) claim ownership of delivery of this care. Ultimately these distinctions do not help advance the cause at a scalable level.
The Institute for Healthcare Improvement has proposed the Triple Aim:
– Improving the patient experience of care (including quality and satisfaction)
– Improving the health of populations, and
– Reducing the per capita cost of health care
The Triple Aim provides a potentially useful framework for considering the implementation of whole person care. Whole person care does attempt to improve the patient experience of care but arguably the degree of one-on-one care suggested by whole person care is not achievable if the healing and curing is to be delivered by the same individual. Even with the growth in heatlhcare as the top employer it is unlikely that enough healthcarers could be trained and employed to provide ‘perfect’ whole person care and reduce the per capita cost of health care.
In this regard I would suggest that we view whole person care from a systems perspective and from the perspective that by introducing systemic change that is oriented to the whole person the Triple Aim could be satisfied.
In a systems approach we could hypothesise that although the ideal might be completed personalised care that there are common values, albeit with cultural variation, that could serve as the basis for interventions that effectively enhance whole person care or patient centre-care but built around change that can be made across systems rather than through training and enculturing of individuals.
Early discussion of a palliative approach may reduce unnecessary admission to intensive care, attempts at resuscitation and other inappropriate care at the end-of-life. Dignity therapy (Chochinov) can improve quality of life and reduce distress and depression. The minimally disruptive medicine approach (Montori) could ultimately translate into reduced use of face-to-face consultations or presentations to emergency care. Minimally disruptive medicine is concordant with our research which has shown that patients with a new diagnosis of cancer, who aren’t immediately terminal, desire normalcy.
So perhaps, there are values, like the desire for normalcy, that can drive system changes to improve the quality of health care but also meet the requirements of the 3rd of the aims, reducing per capita cost of health care. Values of importance could include all of the attributes of patient-centred care as described by Berwick: transarency, individualizaton, recognition, respect dignity and choice in all matters, without exception, related to one’s person, circumstances and relationships in heatlhcare.
The key in taking this approach is striking a balance in the weighting between the ‘values’ recognised by the system i.e. cost, occasions, of service, and sometimes arbitrary metrics of quality, and actual perceived quality of care as described by patient reported outcomes. The current system, specifically in relation to pharmaceuticals, but other aspects of health care, over-rewards in financial terms for small gains in cure and and under-rewards, or possibly doesn’t reward at all, any gains in healing. Health care , cannot only be defined by economic measures and so we should acknowledge that there needs to be some leeway in aligning and balancing economic value with value for the individual – it may be that we can deliver both.
Things they didn’t teach in medical school: Part 27 Managing work-life balance
OK – so many will argue that this is a topic I know very little about…and maybe they are right….or maybe, the way our patient care should be, the truth is that work-life balance should be a very individualized concept.
I know doctors that span the spectrum from their job being part-time and just enough to provide them with an income to pursue their hobbies right through to doctors, for whom, well, work is their hobby and what gives them the greatest satisfaction in life.
I think at the end of the day work-life balance is about finding satisfaction and meaning in day-to-day life and being able to recognize when you need time out from work (or life) to set a balance and recalibrate. For doctors the first step is actually leaving work but the next step is managing time away from work. The big problem for all professions in the 21st century is being ‘always on’. Mobile telephony, SMS, email, twitter, Facebook, and even pagers (remember those) mean that you can be always on. Specific breaks from these points of contact to protect yourself and your family are important – even if you aren’t very good at it (beep….the phone went off again….I wonder who it is).
Whilst I recognize the important of work-life balance of all the things they didn’t teach in medical school this has to be the least formulaic – i.e. maybe it can’t be taught but perhaps there is just advice. Such advice might be – if you have a hobby or an interest then pursue and indulge in it, especially when work is getting you down. And I can’t be prescriptive – maybe you get off on crochet with shaved armpit hair, maybe you are a nude sky-diver (not recommended), you run until you are blue and your knees rebel against your thighs, you grow poisonous plants, play the sitar or in my case listen to 365 different string quartets in a year.
Bottom line is find your own balance.
