Tagged: medical school
Things they didn’t teach in medical school: Part 31 Advocacy
One of the things they didn’t teach in medical school is advocacy. There are different meanings for advocacy – in this case I refer to the broader meaning of advocating for patients and communities to achieve an end to their benefit. An example might be supporting the funding of a new drug or campaigning for increased resources for a hospital.
Simplistically advocacy can just be about being vocal but there can be problems with this approach.
To be an advocate it is important to be able to see all points of view so as being able to bring a cogent argument to the table. Often times advocates are dealing with political situations and positions and invariably these become polarised – it is important to diffuse this polarisation to get the party with whom one is lobbying to also be able to see the arguments in favour of your position. Advocates need to be prepared to compromise to achieve small but important wins rather than overnight revolution.
Advocates need to be careful about their motivations for lobbying. For example it is not uncommon for drug companies to ask doctors to provide support for a new treatment. If this happens there needs to be transparency about the reasons for lobbying and full disclosure of any conflicts of interest.
Similarly advocates need to be careful that their lobbying is not seen as some form of whistle-blowing – this is because some employment contracts prohibit this activity. In this case being part of a community of advocates is important. There is strength in numbers.
There are many tools for advocacy – the main one is conversation and the new medium for conversation is social media. Mastery of social media and branding the advocacy message is a new skill for the medical graduate advocate.
Things they didn’t teach in medical school: Part 28 Keeping up with technology & your patients
One of the things that medical school teaches is the importance of keeping up to date with the latest medical information. Well this is obviously important so that you are administering the most up-to-date treatments. What is not usually included in keeping up to date is keeping up with technology, and importantly, the technologies that your patients will be using. The doctors I know are often early tech adopters in their personal lives but not in work-related use…..healthcare is notorious for its’ slow uptake of electronic health records.
A lot of the technology that has emerged in the last 20 years is only starting to be used routinely in medical practice. Examples include websites to provide health related information or even management, text messaging and emails for communicating with patients, Skype consultations and apps on smartphones. Sometimes we need to take these technologies and use them creatively so that they are more than just electronic versions of paper. For example tablets provide an ideal opportunity to undertake shared decision making activities but more work needs to be done to make this more than eBooks and webpages.
I find the best way to keep up with technology is partly by using it and being an early adopter but also by having diverse information sources. Visual RSS aggregators like Flipboard are great way to find this information, as is subscribing to less than traditional medical journals like The Economist, Wired and Harvard Business Review. The latest place to look is Crowdsourcing websites like Kickstarter and Indiegogo.
Remember….we all like new toys, and some of them are useful.
Things they didn’t teach in medical school: Part 26 – Giving fitness advice
Yesterday I wrote how medical school doesn’t teach much about giving dietary advice. Well the yin to diet’s yang is fitness and exercise. This is also a commonly asked question – what exercise can I do? Is it OK to exercise? Well this is important for both the sick and the well….and I’ll make a confession – I’m not one for formally exercising although my fitbit tells me that generally I do more than 10,000 steps a day.
In some cases it isn’t good to be physically active or to undertake certain exercises like heavy lifting – for example, if you’ve just had abdominal surgery you might increase your risk of hernia. Certain types of exercise – like heavy impact contact sports might be dangerous for a person with bone metastases. But in general keeping active, if not actually exercising is important.
After a stay in hospital many individuals are deconditioned. This happens very quickly with any bed rest – just like an athlete in the off-season. In this case getting back to exercise is very important for return to normal quality of life. There are simple things to do: use a chair for support to stand up between commercial breaks on television, climb back and forth along a small flight of stairs (with a railing) and take progressively longer walks around the neighbourhood (checking out their mail boxes).
Increasing exercise and fitness levels may be important in very specific conditions such as rehabilitation after heart attack or heart surgery, patients with chronic airways disease or after cancer. Increased activity after cancer may actually reduce risk of relapse and prolong life expectancy – the trials are ongoing. Frail and elderly patients may benefit from exercise to reduce falls.
The other aspect of exercise is how to do it. Recent evidence suggests that prolonged periods of exercise are not necessarily the best way of achieving fitness (and weight loss). Interval training with short bursts of intense activity may be more effective. Mixing up different types of exercise might be important for achieving different aims.
Doctors and future doctors need training in giving advice on fitness and exercise.
Things they didn’t teach in medical school: Part 25 Giving dietary advice
One of the commonest questions my patients have is “What should I be eating?”
Interestingly, I don’t think I was taught very much about basic nutrition at medical school. We did learn about the deficiencies such as scurvy (vitamin C) and beri beri (thiamine) but I don’t think we were taught much about normal nutrition. We definitely weren’t taught anything about nutrition in sickness or aberrant nutritional status. This is somewhat unfortunate as most of my patients are either malnourished as a consequence of their cancer or the treatments for their cancer. Living in modern society, most of the remaining people I see are overweight.
Now, you could argue, as the Nutrition Science Initiative does, that we don’t actually know what the ‘correct’ diet is and that most of what has been taught or is understood is wrong, or flawed, but I guess you have to start somewhere. Currently the debate is raging around whether the culprit for obesity is fat, carbohydrates or sugars, or lack of exercise. Various diets – vegan, paleo, Atkins, Mediterranean, etc – argue over the proportions of fat, sugar, carbohydrates, sugars and proteins allowed in the diet. Regardless of the best proportions the fact is that if doctors asked their patients they would soon discover that many wouldn’t know which foods contained what.
Future (and current) doctors need to be taught the best available information about dietary composition and also the behavioural techniques that have been demonstrated to assist in weight loss (or gain). Doctors also need to know how to manage the malnourished patient. Now we can turn to dietitians and nutritionists for advice this is knowledge is so intrinsic to healthcare that it should be considered essential learning. And besides….we might improve the hospital food.
Things they didn’t teach in medical school: Part 22 Project Management #TEDMED
Something not taught in medical school is project management. Although at medical school you might undertake assignments and similar activities, unless you are allocated a research project it is unlikely you will have any formal instruction in project management. I, in fact, don’t consider myself to be especially good at hands-on project management and work better as a collaborator on projects rather than running them directly. Project management is related to time management. You an think of time management as about managing your time to do projects and visa versa project management is a about completing tasks on time.
It is important first of all to recognise a project when it is either handed to you or you come up with the idea.
For me the simplest definition of a project is any activity that can be broken down into smaller tasks to produce an outcome which is more than the sum of the individual parts. Using this definition a project may be small e.g. preparing the meeting roster for a year or large e.g. designing a new medical school curriculum.
There are some tips for managing a project:
– really identify what the purpose and aim of the project is and visualise how the finished project will look – what are the deliverables
– estimate the resources you will need and the time you will need
– identify who is critical to your project – for example, if you need statistics advice for a research project get it early
– break the project down into the smallest tasks possible and work out what in what order they should be completed (and which tasks depend on another tasks being completed – a dependency)
– identify what will stop the project from being finished
– based on the above decide if your project is feasible or not
– identify stakeholders and collaborators
– once the project has started have a regular review process to check progress
Last night at the opening session of TEDMED 2013 Professor Rafael Yuste spoke about the relationship between pursuing big science and his passion for mountaineering. He broke them both down to 3 steps: assemble the team, map the course and keep the summit in sight. The scientific summit he plans to climb is the Brain Activity Map now known as the Brain Inititiative which was announced by Barack Obama 2 weeks ago. This is the moon project or human genome project of the decade. You can see him talk @TEDMED
Things they didn’t teach in medical school: Part 21 – you can do more than look after patients
So I don’t really like the title I came up with, after all, looking after patients is pretty important. What the title refers to is the observation that medical training equips you for more than medical practice – although nobody teaches you that.
I haven’t quite reached the point of abandoning face-to-face patient care but increasingly I spend my time undertaking activities that might be considered influencing care rather than undertaking care.
It is often observed that many people with law degrees don’t end up being day-to-day lawyers. Well this probably applies to a lot of the core professions. Last week I ran into a basic scientist who now has a job as a research strategist and commercialisation advisor.
So what is the common theme?
Professional training really consists of two themes. One is largely around the technical knowledge relevant to the discipline – i.e. the law for lawyers, economics for economists, anatomy/physiology/pharmacology for doctors, etc, etc. The second is around problem solving. Professionals/experts fundamentally have the job of correctly identifying problems and questions and then trying to solve them. In medicine my job is to ‘diagnose’ the patient’s illness, prioritise the management problems and solve them.
Now, as I sit on hospital administrative committees and company boards, my job is the same. Identify the problem and find the solution.
This week an end came to an advisory committee that I have sat on for the last 6-7 years. The advice was around eHealth and electronic decision support. Whilst I do have some understanding and technical knowledge of these areas my real contribution to the group was to look at problems from a different perspective, to re-define the problems, to re-calibrate the discussions. This was also the role of my fellow committee members who were often drawn from different professions or different versions of my profession.
Some of my colleagues and peers make a complete jump and leave day-to-day medicine altogether to pursue apparently different careers. I’m pretty sure they are out there diagnosing problems and finding solutions.
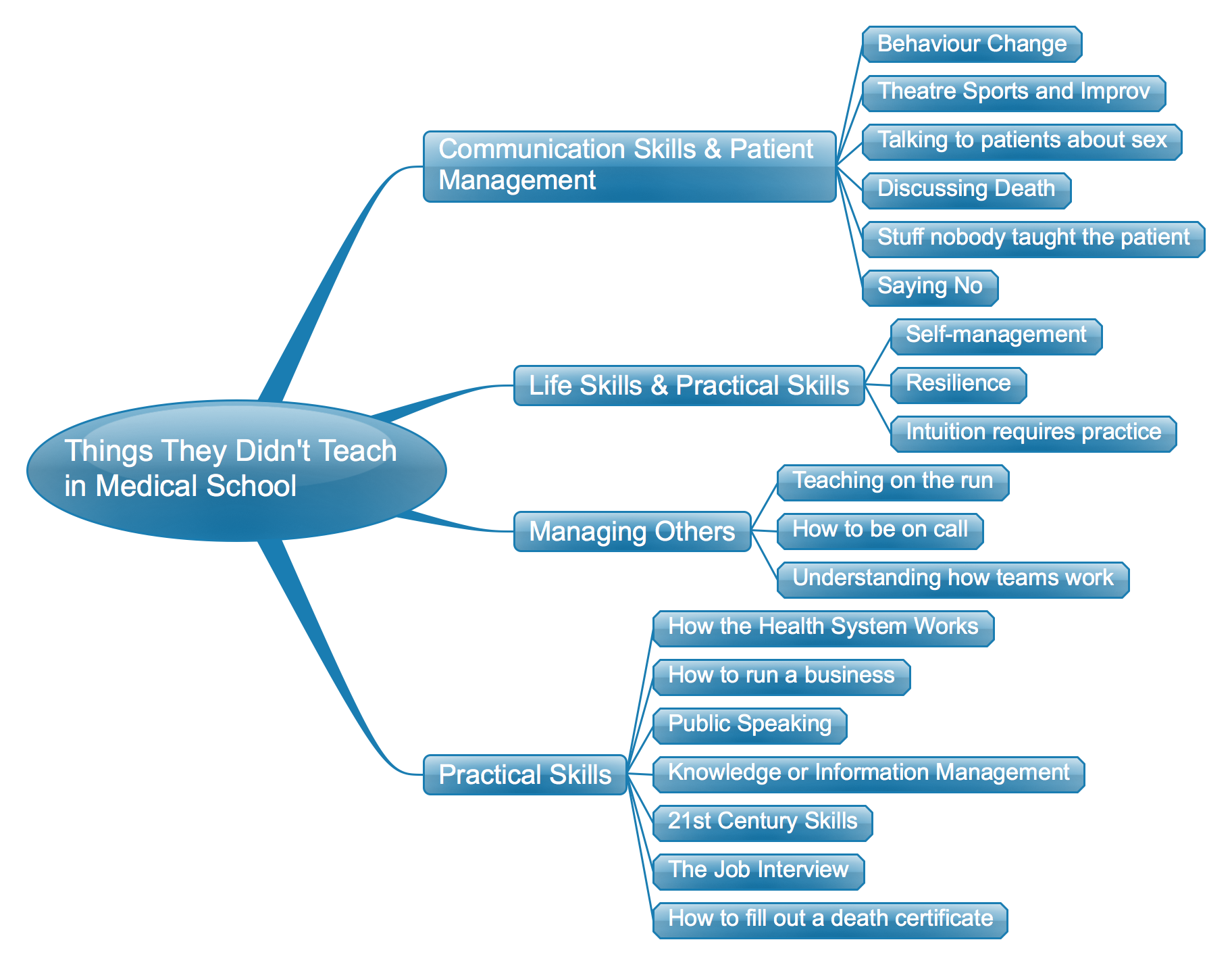
Things They Didn’t Teach in Medical School: The list so far – a mind map
Things they didn’t teach in medical school: Part 10 Talking to patients about sex
It’s always the last thing that comes up in the consultation. You’re sort of winding up and your patient says “I’ve just got one more, um, question”……followed by a pregnant pause. “Well it’s been 3 months since the operation and I haven’t been able to get an erection”. This is basically how recent conversations with some of my rectal cancer patients has started. Unfortunately for many of these patients – after cancer, chemoradiation and then pelvic surgery there might never be a recovery and pharmaceutical aids like Viagra may not help. Some get a slow recovery over time as their pelvic nerves recover. The problem affects both young an old.
The reasons for sexual dysfunction are many and varied and range from physical incapacity to altered body image. In my peritonectomy patients has shown that men can experience erectile dysfunction and women can experience pain, difficulty lubricating an achieving orgasm. Many patients are concerned about sex when they have a stoma bag and women are often concerned about urinary leakage. In some cases patients have heard myths about it being unsafe to have sex after cancer or their health carers have given them overly cautious instructions about intercourse whilst on chemotherapy.
My communication skills training never covered this scenario. It’s even worse when the discussion is not just about the ability to perform sexual intercourse but also the issue of fertility. For younger people we do often discuss implications for fertility and might recommend sperm banking in men or various fertility treatments for women but more often than not sexual ‘side-effects’ are an afterthought. We aren’t actually taught much about how to treat these side effects nor are we instructed how to deal with the issues between couples. I’m sure part of the problem is society as a whole isn’t great at talking about these things so doctors are behind the eight ball to start with.
Talking to patients about sex is something we have to learn after medical school and the best way to do it is just try and relax and be frank about the issues.
For more on this topic see the NY Times blog post by Suleika Jaouad Life, Interrupted: Crazy, Unsexy Cancer Tips
What they didn’t teach in medical school Part 2: how the health system works
One of the things that wasn’t taught well when I went to medical school was actually how the health system works: in my case I’m referring to the Australian health care system but I’m sure the sentiment applies in other countries. Knowing how the health system works overlaps with how to run a business, which I’ll cover in a later post.
When you are studying medicine and even once you’ve graduated and working in the hospital you don’t really pay attention to how the health system works. The patients come and go and you do your best to look after them. It’s perhaps only once you actually have to go out and get a job, either in the hospital system or in private practice, that you start to care. When I refer to ‘how the health system works’ what I really mean is ‘how is health care paid for’. Once you get a job you are concerned with how you are paid and/or will pay other people. If you work in hospitals then you spend a lot of time listening to other people tell you you can’t do stuff because there is no money – even if what you want to do will result in real improvements and maybe even save money at the end of the day.
In Australia it is becoming even more important for medical students and junior medical officers to be taught how the health system works. As a result of the last round of health care reform the Federal government is phasing-in activity-based funding. So hospitals will be based on what they do according to a National efficient price. This sounds straight forward but in practice it is much more complicated. Hospitals won’t necessarily be getting paid on the basis of the activity they undertake. Governments must allocate budgets from finite coffers so the money local hospitals receives is based on projections, somewhat spuriously called targets. If the hospital undertakes more activity than predicted then unless it operates very efficiently it may end up over budget.
Medical students, junior and senior medical officers need to know about how activity-based funding works as they are the source of the the documentation about how much activity is being undertaken. Unless the doctor records not only the cholecystectomy but the co-morbidities of the patient and complications incurred during the hospital stay then ultimately the coding of the data to obtain funding will be inaccurate and inadequate. This in turn leads to inadequate models upon which the hospital activity targets are set.
These processes and in evolution and being rolled-out over the coming years. Doctors and their students need to become more familiar with how the system works so they can influence how their hospitals or practices are run and how the money is spent. Knowing how the system works will change how doctors work. Health care practitioners also need to be aware developments in primary care, such as the development of Medicare Locals. They will also need to keep up to date and the system is likely to change again. This is the decade of activity-based funding in Australia. The next decade might see a shift to process and outcomes-based funding and further changes to the way doctors practice.
I’ve only touched one major aspect of how the health system works. In Australia it is very complicated due to Federal, State and Local considerations. Medical schools will need to teach according to their local health care environment.
For more information see Activity Based Funding and the Independent Hospital Pricing Authority
