Philip Glass Symphony No.9
What they didn’t teach in medical school Part 1: Behaviour Change
This is the start of an occasional series about stuff they didn’t teach me in medical school – and I suspect they still don’t teach this stuff. Where it was taught I suspect it was pretty poorly. These musings have come about because most of what I do now, that doesn’t fall into the categories of diagnosing or treating, wasn’t taught in medical school or as part of my specialist training. Some of these things include how to be an administrator, how to run a meeting, how to run a business, how to teach trainees and a whole bunch of stuff around fine-tuning the practice of medicine. I won’t necessarily have the answers about what to do to address these problems but recognition is the first step.
To kick it off with I’m nominating how to change patient behaviour.
Most of what I do on a day to day basis as an oncologist is prescribing medications to treat cancers. But there are a whole lot of behaviours that might also need to be changed or created to help my patients get through their illness. In the same way primary care practitioners need to be able to help their patients change behaviours in order to achieve preventative medicine goals.
Examples of behaviours and problems that might need to be addressed through behaviour change include tobacco, alcohol and substance abuse, obesity and poor fitness, poor adherence to medications or aberrant mechanisms for coping with illness.
I recall being taught how to detect these problems but not a great deal about how to address them. I suspect most busy doctors see their patients and go through the motions of discussing smoking cessation or some other behaviour change but either give up in despair or through lack of time or perhaps take the easy option and write a script for a patch or some other aid (which might help but should be part of a package deal not a one stop solution).
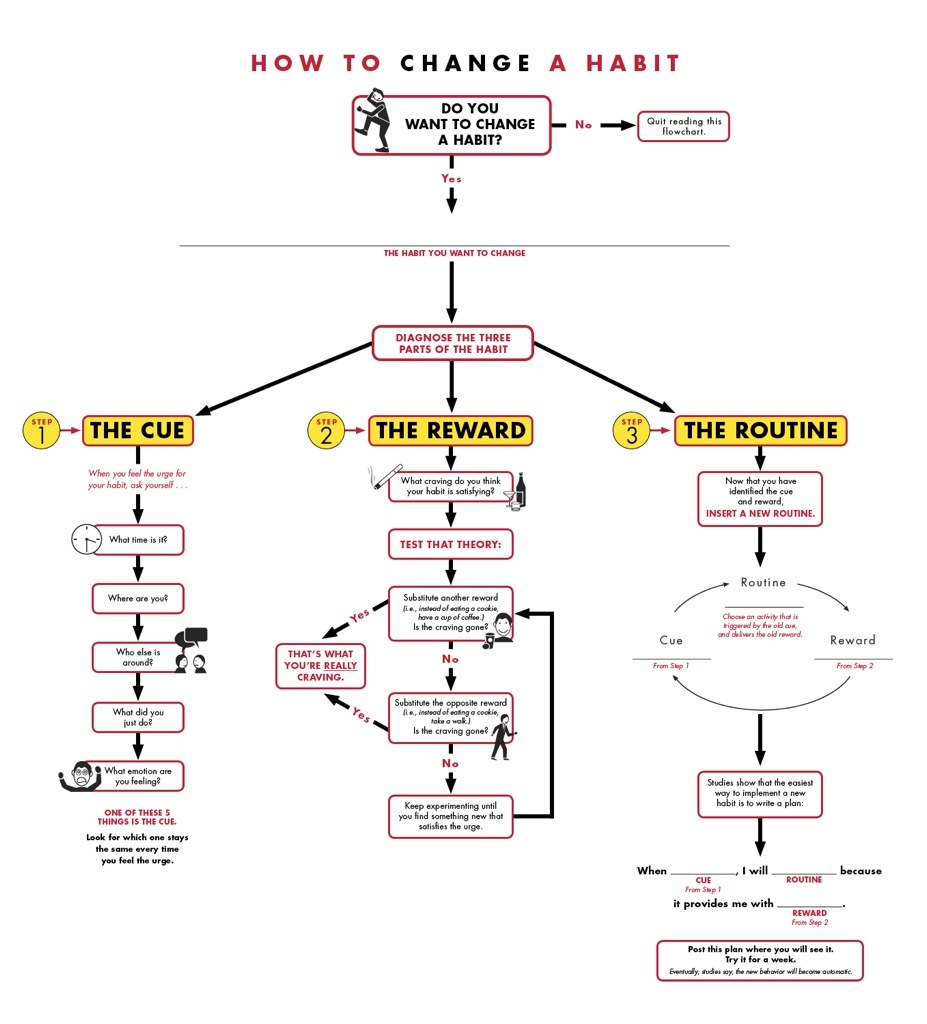
So every doctor dealing with these problems ought to read up or take a class on behaviour change. It’s all the rage in popular non-fiction right now with books on behavioural economics (Nudge by Thaler & Sunstein, Thinking Fast and Slow by Kahneman) and habit change (The Power of Habit by Duhigg) being in the best-seller lists.
If you’re a doctor reading this then one way to learn about it is to try and change one of your own habits. Here a some clues how Charles Duhigg Habit Change Resources
Zoomusicology – is it for the birds?
Listening to Jonathan Harvey Bird Concerto with Piano Song played by Hideki Nagano with the London Sinfonietta conducted by David Atherton. For more on this work see Bird Concerto
You might also like The Piccolo and the Pocket Grouse
Edgard Varese Ameriques (1927)
Michael Tilson Thomas conducting San Francisco Symphony in Ameriques by Edgard Varese.
For more info see Ameriques
A New Year of Music
After a relative year off having completed the 365 String Quartets in 2011 I’m kicking off the musical journey again with an emphasis on modernism, 20th Century & contemporary classical orchestral music. To be liberal about the 20th Century I’ll listen from the period of Brahms & Mahler to the present.
Kicking off the year is Detailed Instructions (for Orchestra) 2010 by Nico Muhly, played by the New York Philharmonic under the direction of Alan Gilbert.
The Curator Unplugged – Training Future Doctors in the Era of Electronic Decision Support
One of the key problems facing educators in medicine today is how to train future doctors in medical decision making in an emerging era of electronic decisions support in EHR (electronic health record).
Let’s look at the transition that is occurring.
In the traditional model of care the doctor is presented with diagnostic and management problems by a patient. The doctor gathers information to make this decision. The doctor does this by history taking, physical examination and selection of tests that will aid him/her in the decision making process. In some, perhaps many circumstances the doctor will need to seek additional decision aids. These decision aids were originally hard copy textbooks, journals and guidelines but now are accessed online. The decision making process combines automatic responses learning through repeated observation and practice and critical reasoning hopefully informed by the best available evidence.
In the new model of care the history and examination are entered into the EHR. The EHR can then act as an iterative decision aid. It may suggest an order set of tests based on the history and examination. When these results are available it may in turn suggest treatment pathways or modification to treatments e.g. in guiding antibiotic dosing based on renal function derived from blood results. The EHR becomes a 3rd party in the decision making. To add to the complexity the patient may be more engaged than ever before. The patient may have contributed their history electronically and be armed with a list of differential diagnoses and treatment options derived from research conducted on the internet.
In the new model of care the processed leading to the decision are apportioned differently. The formulation of initial impressions may be supplanted by algorithms. Electronic decision support may provide some advantages in terms of standardization of practice leading to quality and safety improvements. Equally so, for a long time, the algorithms will not be artificial intelligence. The role of the medical practitioner must become one of knowing when following the algorithms is appropriate and when the system needs to be overruled. The doctor, or nurse, needs to be able to justify this and also explain to the patient why they are bypassing the system. Indeed, the role of the medical practitioner, more than ever before, moves from being the source of truth to being the filterer of options and the explainer of decisions. Practitioners will need to be able to promote health literacy in their patients in order to allow them to use the information they have found on the internet.
When I originally started thinking about these problems I thought simplistically of the doctor as a knowledge managed collating the necessary data needed to make medical decisions. In the EHR-enabled environment this would appear, at face value, to become easier. In reality the role is greater than collector it is one of curator. The curator must work with their environment, the EHR, and use both system 1 and system 2 (see Thinking, Fast and Slow by Daniel Kahneman) to make decisions. Currently, physicians who have trained in the traditional methods may actually frown upon use of electronic decision support but they may be better equipped to use it than the doctors of the future. If the doctors of the future are trained in an environment of instant decision support they may fail to gain the clinical experience necessary to recognise when the algorithms are inappropriate. The doctors of the future may be buttressed by electronic decision support but might have less capacity to deal with more complex problems and decisions simply by virtue of not having at one point sweated on the easy stuff. Their medical system 1 may not have grown enough to allow the best use of system 2.
Frank Davidoff compares physicians to musicians declaring that “clinical practice is above all a matter of performance” (Ann Intern Med. 2011;154(6):426-429). If this is the case then the training doctors of the future will need to spend at least some of their time ‘unplugged’ from the eletronic decision support in order to hone the skills needed to perform medicine at the highest level. Trying to establish the right balance will be the challenge for the medical educators of the future.
Training prescribers how to prescribe mHealth apps
Sometime soon your doctor is going to prescribe you a mHealth app for your smartphone. There’s a 1 in 3 chance you already have one on your phone – for tracking calories, weight, exercise, your smoking, your blood sugar or our mood. How will you or your doctor know which is the right app?
Well at the moment nobody really knows. Intuitively, tracking your health with apps might help you to achieve your health goals but strictly speaking nobody really has built the evidence-base. In fairness to the evidence builders, the iPhone has only been around for 5 years and “there’s an app for that” was first used on Jan 29, 2009. Preliminary evidence suggests current mHealth apps aren’t really designed for health promoting behaviour change http://www.jmir.org/2012/3/e72/
Nonetheless, the market is out there. Happyique is already piloting a portal for app prescriptions…..reimbursement for prescription to follow http://www.happtique.com/mrx/
Your doctor hasn’t been trained in health behaviour change – this is a new job for medical school. Standards are needed – Happtique has started this work – they need to be grounded in evidence and sound from the perspective of psychology and behavioural economics.
How to move forwards? Teach medical student about behaviour change. Regulate apps according to evidence but with a light touch. Teach consumers to find reputable, independent apps.
Read more at http://www.nytimes.com/2012/08/20/technology/coming-next-doctors-prescribing-apps-to-patients.html?pagewanted=all
Will your doctor be prepared to override you and your smartphone?
It is your classic sci-fi scenario. Remember HAL? Remember the synthetics in Alien(s)? Well now there is a storm brewing that will dramatically change healthcare. This change is coming due to the convergence of a number of trends in healthcare and a few disruptive technologies, of which the most important is the smartphone.
The key changes are:
- patient use of the internet to obtain health information and make healthcare decisions
- the slow but inexorable rise of electronic health records (EHR)
- digital modes of communication between patients and healthcare providers
- the development of knowledge repositories for electronic decision support
- the use of behavioural economic techniques, social media engagement and analytics, gamification and other methods to modify health behaviour. This change is epitomised by the life-logging, quantified health movement
- the development of sophisticated diagnostic devices for personal use
Patients have been empowered by the internet. They come to my office clutching folders of printouts from the internet or hold-up their iPad for me to see what they’ve found. Some of this information is good and much extremely bad. Some patients handle this information well and a lot don’t have the health literacy skills to filter the good from the bad. A lot of my time as an oncologist is spent interpreting this information for patients, often after they’ve already spent a lot of money on dodgy treatments.
Electronic health records are already widely used, especially in primary care. EHR are increasingly integrated into hospital care. But these are disjointed. The next 10 years will see EHR start to be able to talk to each other to provide seamless transitions between healthcare settings. In Australia this will be built around the PCEHR. Ultimately cradle-to-grave healthcare data will be held in a cloud-based repository accesible by patients and their healthcare providers.
Communication between patients and their healthcare providers has been changing. Face-to-face is being supplemented with email, video calls and text-messaging. Doctors are remotely visiting patients in hospital by video enabled robots. Patients book appointments with doctors via mobile apps.
EHR can be more than an interface for a data repository for patients. Electronic decision support can be built into EHR to aid in the delivery of evidence based health care. Electronic decision support provides a knowledge base and rule book for quality and safety, particularly in relationship to prescribing. Linking patient data with analytics and knowledge repositories will not only takeover large chunks of patient management, especially in he hospital setting, but will also be capable of learning and improving care. Big data will be analysed for emerging health trends.
The quantified-self movement is slowly becoming mainstream. Life-logging relatively easy to measure end-points such weight, exercise and caloric intake is a simple means for managing weight. Assisted by mHealth apps on smartphones and tablets individuals can take their own control. Support through gamification and social networks may increase adherence and success in achieving health goals. Numerous other applications such as smoking and alcohol control, sleep management and habit changing are possible and already being undertaken.
Finally new diagnostics devices are emerging for the collection of health care data. The Holy Grail is the medical tricorder concept from Star Trek. This device is used to scan the patient and produce a medical diagnosis and provide treatment recommendations. How far away is this? The folk at Scanadu http://www.scanadu.com have a 12-18 month time horizon pending FDA approval. These devices will draw on and consolidate many aspects of the preceding 5 ideas.
So imagine you are at home. Your love one feels sick – or maybe your ginger.io app tells you you are becoming sick. You scan your child and a diagnosis of an infection is made through analysis of combination of scanner data and manually (voice) entered symptoms. The software may also have trawled social networks and hospital data to identify common infections in your community. A diagnosis is provided that says your family member needs antibiotics and you should see a doctor for confirmatory tests and a prescription.
Here is where it gets tricky…..What if the doctor disagrees. Who do you trust? The interweb or the experience of the doctor? What if the doctor runs his own scan and his software from a rival company comes up with a different recommendation? Will the doctor overrule the software? What if the doctor is wrong and the software is right – or visa versa? Who is responsible? We wan’t patients to take responsibility for their health but will they take responsibility for their healthcare decisions? And hey, if the software is right – do we cut out the doctor – does a doctor in the cloud get to prescribe the antibiotics?
This technology is an awesome step-forward for healthcare, especially as the price of the technology will allow scalability even in low income countries.
But is the healthcare system ready…..not even close.
Are the patients ready…..less than they think.
Even if initial uptake of tricorder technology is slow the need for regulatory management will be urgent.
Where are the opportunities? Developing robust knowledge bases. Suppporting data and decision support standards. Teaching people how to use the tech to support their healthcare decisions and to Be Medicinewise. And developing new models of electronic and human-based healthcare delivery.
Re-booting the blog
Have been quiet on the blogging front since the Year of the String Quartet 365SQ. Have migrated across from Posterous and plan regular commentaries on health care with an emphasis on personal and personalised medicine, healthcare practice change, oncology, eHealth, and medical education, and the occasional excursion back to music – so watch this space.
