Tippett Symphony No.4
Symphony No.4 by Sir Michael Tippett played by Chicago Symphony Orchestra conducted by Sir George Solti
Symphony No.4 by Sir Michael Tippett played by Chicago Symphony Orchestra conducted by Sir George Solti
So perhaps this should have been part 20.
Assessing one’s own performance as a doctor is not taught at medical school.
The problem is of course that as a doctor there is a touch of the ‘God’-complex, not to mention a historical lack of scrutiny.
But on a more personal note it is actually very difficult to step-aside and assess your own performance objectively.
One way to do this is to focus on how you handled the difficult case. But in reality the difficult case was probably going to be difficult regardless of how brilliant a clinician you are and in many circumstances the reasons why the case is difficult is out of your control.
I think the real challenge is assessing overall performance. A little like assessing organisations you can assess processes and outcomes. Outcomes are the difficult measure because you don’t necessarily know how your peers perform and different doctors treat patients with different ‘degrees of difficulty’.
For both process and outcomes you can assess against benchmarks and guidelines but there will always be uncertainty about how these are set.
Finally one needs to have a personal reference point: do you aim for a consistent standard within a specific set of skills or do you have a reference of achieving both this, combined with progressive improvement & expansion of your skill-set.
I think the latter is the most important issue that needs to be addressed before the profession can embrace personal self-assessment. Do the practitioners know what their goals are? Do you graduate and coast or graduate and grow? Self-assessment needs concrete actions otherwise others will do it for us and no doubt in a way that won’t be helpful.
Lorin Maazel conducts the New York Philharmonic in Mahler Symphony No.4
http://en.wikipedia.org/wiki/Symphony_No._4_%28Mahler%29

Sir Michael Tippett Symphony No.3
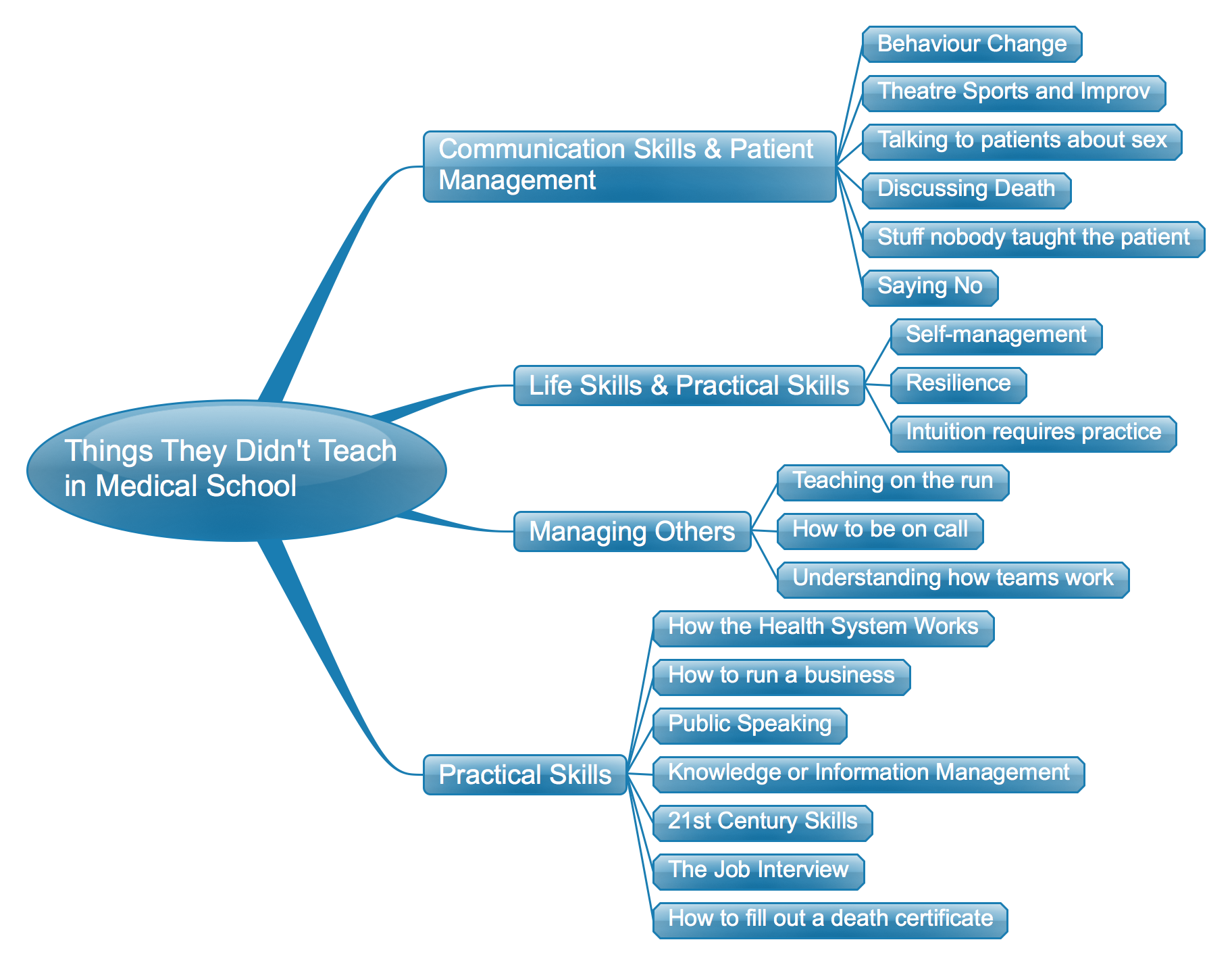
One of the things that isn’t taught in medical school is how often one needs to say ‘no’ and how to go about doing it.
There are different types of ‘no’.
There is ‘no you are wrong’, ‘no, that is inappropriate treatment’, ‘no you don’t understand what you’ve read on the internet’ and ‘no, I can’t do that because it is unethical (or illegal)’….to name a few.
Almost always saying ‘no’ is telling somebody just the thing that they don’t want to hear or aren’t prepared to hear. The trick to saying ‘no’ is avoiding that person going to another doctor who will tell them what they want to hear. More often that not that doctor will not have worked out how to deal with the difficult situations created by needing to say ‘no’.
Medical schools can help future doctors by teaching them to identify these situations and teaching them how to say ‘no’.
Michael Tippett Symphony No.2 Sir Colin Davis and the London Symphony Orchestra
Michael Tippett Concerto for Double String Orchestra – Academy of St.Martin in the Fields conducted by Sir Neville Mariner
Trawling the web and social media I’ve come across a fascinating community of individuals interested in death and death-care. The spectrum of discussions is broad, ranging from advanced care directives, through death midwifery and to designer garments to take to the grave. This has led me to think about how my patients die.
Some, but actually not many patients die at home with their families. Sadly, some die at home with nobody. Many die in hospital or hospital-like settings including hospice. More often than not there is a small single room which is quickly cramped when more than 2 or 3 family and friends are present. Especially in hospitals it is very medical and not very individualised right up to the end. Not much of the person is evident in these rooms.
I’m not really sure why this is the case. Perhaps the patients are too sick to direct their care or maybe we perceive them to not be interested in the usual things of life.
Palliative care focuses on preventing and relieving suffering and is effective therapy for dying people. But palliation seems to have been framed largely from the perspective of maintaining quality of life and alleviating symptoms rather than pursuing a hedonistic approach. By this, I mean, we don’t pay much attention to the provision of pleasure and pleasurable experiences for the dying person. This is despite recent literature from the dignity therapy movement suggesting the importance of pleasure for the dying person.
Our cemeteries have water views and garden vistas but our living dying do not. Julian Barnes has said “We spend time thinking about our funeral music; less about which music we wish to do our dying to”. For those that can still eat and drink we provide unpalatable hospital food and often deny them the beverages of their choice. We sometimes think about specific ethnic needs but we don’t think about sub-cultural needs – dying in familiar surrounding for the outdoors person or the Goth. Maybe the dying don’t want to be dressed in backless white gowns but would prefer their own clothes, maybe even dress for the occasion one last time.
So maybe there is a place for designer death-care. Personalised services might help people at the end-of-life not only die with dignity and without suffering but also with maintenance of identify and experiences of pleasure right to the end. Existing practitioners could incorporate into their rounds the question – has anything brought you any pleasure today? what could we do to bring you some pleasure?
Pursuing a palliative approach is good – pursuing it with a pinch of hedonism might be better.
http://www.orderofthegooddeath.com/
http://www.engagewithgrace.com/
Karl Bohn & Staatskapelle Dresden play Strauss: Ein Heldenleben Op.40 and Tod und Verklarung Op.24
