Category: Medicine
Things they didn’t teach in medical school: Part 20 How to do meetings
So over the weekend I speed read Sheryl Sandberg’s book Lean In.
I was motivated by the useful summary by the NY Times David Brooks: “Think about Sheryl Sandberg’s recent book, “Lean In.” Put aside the debate about the challenges facing women in society. Focus on the tasks she describes as being important for anybody who wants to rise in this economy: the ability to be assertive in a meeting; to disagree pleasantly; to know when to interrupt and when not to; to understand the flow of discussion and how to change people’s minds; to attract mentors; to understand situations; to discern what can change and what can’t”.
This reminded me about something that is increasingly important in my life – going to meetings. In fact my colleagues give me a hard time because I’m a bit of a meeting junkie but this is only because they spend 4-5 hours a week in meetings as opposed to my 20.
If as a doctor you work in a hospital and you are engaged with the running of the place you will need to spend a lot of time in meetings. These range from meetings of 2-3 people to 20 or more. The reasons for the meetings will be diverse and they encompass education, environmental scanning (FYI meetings), working meetings (i.e. you are making decisions) and advisory meetings (where you are helping others make decisions).
There is a lot written about how to run effective meetings so I won’t re-iterate all of these writings. I will say however that you need to know what the purpose of the meeting is and at the end of any meeting there needs to be an outcome…a decision or an action arising. Bad meetings are staccato and without resolution whereas good meetings have ‘flow’ and resolutions. Meetings work when everybody who wants a say gets a say, diversity of opinion is expressed and the outcomes are determined by consensus (this doesn’t actually mean everybody likes the outcome but everybody agrees).
Overall David Brooks’ summary offers a nice approach to meetings.
One final thing you do need to know about meetings is when to say no….my rule is that unless it is exceptional there is no role for ‘routine’ meetings that happen only twice a year….almost by definition these don’t achieve anything.
There is a whole additional art to chairing a meeting – one which I’m just coming to grips with – and which will form another post.
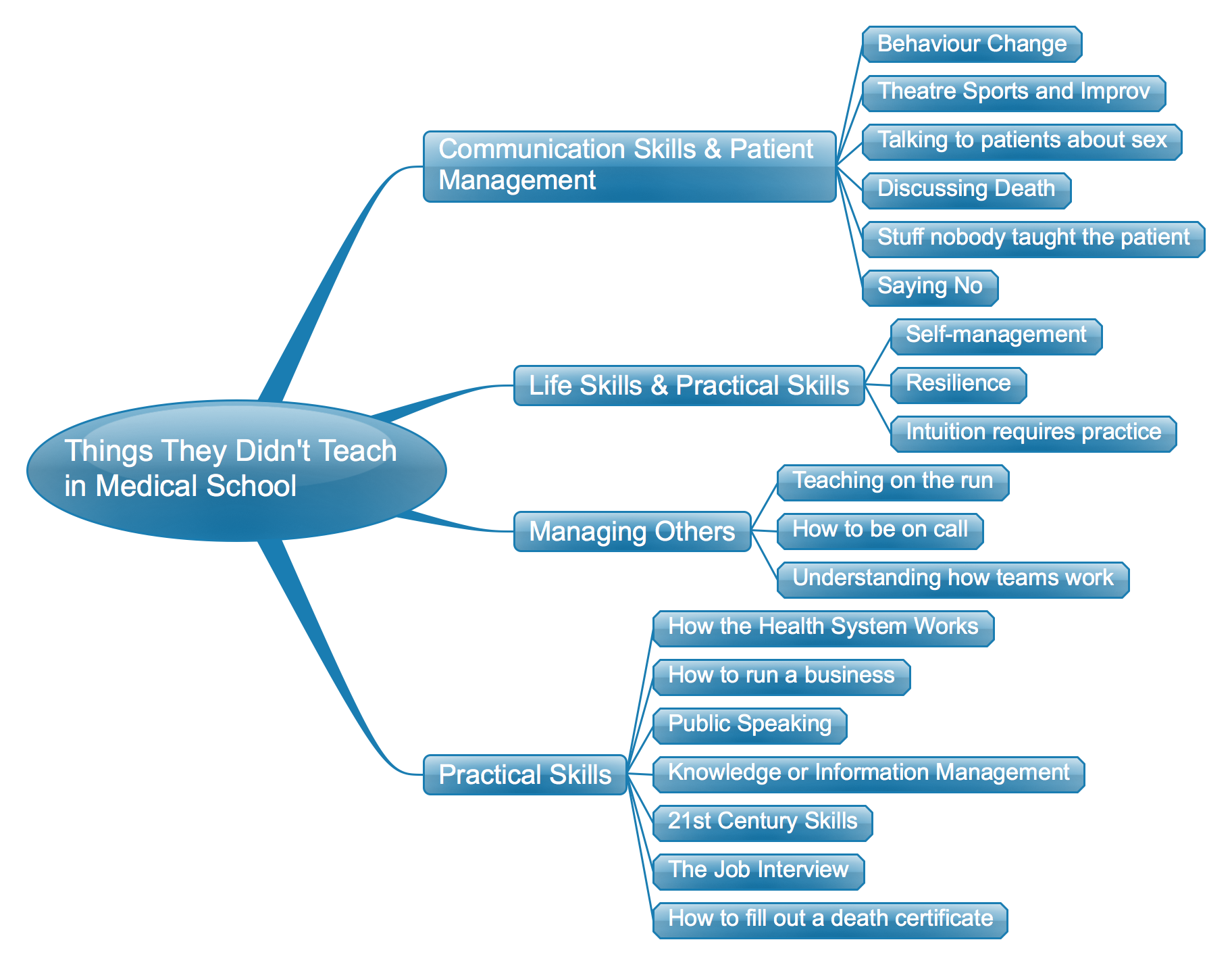
Things They Didn’t Teach in Medical School: The list so far – a mind map
Things they didn’t teach in medical school: Part 19 Saying No
One of the things that isn’t taught in medical school is how often one needs to say ‘no’ and how to go about doing it.
There are different types of ‘no’.
There is ‘no you are wrong’, ‘no, that is inappropriate treatment’, ‘no you don’t understand what you’ve read on the internet’ and ‘no, I can’t do that because it is unethical (or illegal)’….to name a few.
Almost always saying ‘no’ is telling somebody just the thing that they don’t want to hear or aren’t prepared to hear. The trick to saying ‘no’ is avoiding that person going to another doctor who will tell them what they want to hear. More often that not that doctor will not have worked out how to deal with the difficult situations created by needing to say ‘no’.
Medical schools can help future doctors by teaching them to identify these situations and teaching them how to say ‘no’.
A Hedonistic Approach to Palliative Care and Designer Death-care
Trawling the web and social media I’ve come across a fascinating community of individuals interested in death and death-care. The spectrum of discussions is broad, ranging from advanced care directives, through death midwifery and to designer garments to take to the grave. This has led me to think about how my patients die.
Some, but actually not many patients die at home with their families. Sadly, some die at home with nobody. Many die in hospital or hospital-like settings including hospice. More often than not there is a small single room which is quickly cramped when more than 2 or 3 family and friends are present. Especially in hospitals it is very medical and not very individualised right up to the end. Not much of the person is evident in these rooms.
I’m not really sure why this is the case. Perhaps the patients are too sick to direct their care or maybe we perceive them to not be interested in the usual things of life.
Palliative care focuses on preventing and relieving suffering and is effective therapy for dying people. But palliation seems to have been framed largely from the perspective of maintaining quality of life and alleviating symptoms rather than pursuing a hedonistic approach. By this, I mean, we don’t pay much attention to the provision of pleasure and pleasurable experiences for the dying person. This is despite recent literature from the dignity therapy movement suggesting the importance of pleasure for the dying person.
Our cemeteries have water views and garden vistas but our living dying do not. Julian Barnes has said “We spend time thinking about our funeral music; less about which music we wish to do our dying to”. For those that can still eat and drink we provide unpalatable hospital food and often deny them the beverages of their choice. We sometimes think about specific ethnic needs but we don’t think about sub-cultural needs – dying in familiar surrounding for the outdoors person or the Goth. Maybe the dying don’t want to be dressed in backless white gowns but would prefer their own clothes, maybe even dress for the occasion one last time.
So maybe there is a place for designer death-care. Personalised services might help people at the end-of-life not only die with dignity and without suffering but also with maintenance of identify and experiences of pleasure right to the end. Existing practitioners could incorporate into their rounds the question – has anything brought you any pleasure today? what could we do to bring you some pleasure?
Pursuing a palliative approach is good – pursuing it with a pinch of hedonism might be better.
http://www.orderofthegooddeath.com/
http://www.engagewithgrace.com/
Things they didn’t teach in medical school: Part 18 Intuition Requires Practice
The dogma of modern medicine is that it should be evidence based. Well this is true but in actual day-to-day practice the evidence is often only marginally helpful.
In actual fact we practice a lot of medicine based on gut instinct. And this gut instinct is learned from doing the same thing over and over again, by seeing similar cases and recognising what the outcomes will be. This is a type of evidence based medicine which we might call experience based medicine.
Let’s tale the example of dose-adjusting chemotherapy. There are guidelines about what to do but when you take a phone call you invariably don’t look up a guideline. I adjust the doses partially based on guidelines and mostly based on my experience of what will happen with dose adjustments. The reality is that practice makes, if not perfect, at least better.
When can I claim CPD points for my blogging & microblogging?
Continuing profession development or continuing medical education concerns a number of activities aimed at maintaining professional standards, skills-based competency, and currency of knowledge and practice. I’ve just lodged my 2012 CPD points with the RACP. 100 points are required over 12 months. These points are relatively easy to accrue for somebody like myself, for example, attending a conference might garner between 10 and 30 points, a publication scores 5 points, post-graduate study carries 50 points a semester. You can acquire points through online learning, logging your access of UpToDate, recording the clinical meetings you attend and teaching undertaken, and logging participation in quality improvement exercises.
One of the key points with CPD is reflective learning. In fact, in the program that I participate in, demonstrating reflection garners additional points.
After submitting my points I realised that I didn’t include my blogging and microblogging as part of my CPD and likewise – there was no category for this type of activity in the menu of options available to accrue points. When I post medical tweets it is often after having read abstracts and whole articles from the medical literature – these days often through Read by QxMD on iPad, via the popular press such as the New York Times, or several other healthcare blogs. My tweets become a potentially audit trail for my CPD activities.
My blog posts have largely been reflective learning pieces on ‘things they didn’t teach at medical school’ and commentary on health policy issues, in particular, on eHealth.
Reflective writing is increasingly adopted into medical school curricula and part the formative assessment process of students. Fischer et al found no difference between written and blogged reflections undertaken in medical clerkships (Med Educ 2011 45(2):166-75).
Although CPD is largely inwards looking blogging and microblogging serve an outward looking purpose in that it is a way of disseminating information and opinion and also communicating with other interested parties, potentially creating learning communities. In some cases the amount of influence is measurable through a variety of social media metrics (e.g. Klout and Kred Scores).
CPD programs should recognize blogging and social media activities as valid forms of reflective learning.
Things they didn’t teach in medical school: Part 15 Resilience
1 in 5 physicians experiences emotional, psychological and physical damage related to burnout. The corollary to this is that many don’t experience burnout and manage to prevent it – why might consider these individuals to be resilient. Resilience should be taught in medical school and doctors need to recognise burnout in their peers and other staff.
Resilience can be defined as the “capacity to respond to stress in a healthy way such that goals are achieved at minimal psychological and physical cost”, i.e. in other words resilient individuals have the capacity to bounce back after stressors and set backs and potentially be stronger.
The current issue of Academic Medicine 2013 (88) has a nice article by Zwack and Schweitzer and an accompanying editorial by Epstein and Krasner that respectively identify and discuss the characteristics of the resilient physician:
– mindfulness
– self-monitoring
– limit setting
– & attitudes that promote constructive and healthy engagement with difficult challenges at work (rather than withdrawal or avoidance)
Some of these characteristics are teachable or coachable and should be considered as manatory in medical school.
Things They Didn’t Teach in Medical School Part 13: Understanding How Teams Work
Well this is a half truth. Teamwork is emphasized at medical school. But is it really taught the way it works in the real world. It is more theoretical than real In medical school you do team based exercises but these are largely with peers. In hospitals and other healthcare settings there is a mix – doctors, nurses, allied health and all of differing levels of seniority. And particularly in the hospital system there is pretty constant turnover of junior staff.
We examine the competency of individuals but not of teams or competency within a team.
Teams can become dysfunctional if there is one bad player or sometimes they continue to excel despite a poor team player – nobody really knows why.
For me the key issues are clear roles, inter-team member support (the buddy system) and a common purpose.
The Australian Local Health District Paradox or How Does One Assess LHD Board & CEO Performance
National Health Care Reform, and in fact all of Australian government, is built around the principle of subsidiarity – i.e. that delivery and implementation of services, and decisions concerning services should be made as close to the ‘coalface’ as reasonably possible. This has resulted in the creation of local health districts or LHD. The LHD receive a mixture of State and Federal funding that is predominantly administered through State ministries. The LHD governance consists of a Board and a CEO with his/her executive team.
The remit of the LHD Board is to ensure good management of the district and philosophically the Board must protect, and indeed pursue, the interests of the local community. At inception the CEO were appointed by the States rather than by the Boards and the Chairmanship of the Boards, albeit voluntary, was also essentially at the discretion of the States.
The CEO has in effect two masters – the State Ministry of Health and the Board. The CEO is bound to try and achieve the performance targets set by the State. At the current time these are largely around activity based funding. The CEO and Board and hospitals must bring the budget in on target.
The problem for hospitals and their Boards is that hospitals new improvement, renovation and redevelopment. States tend to do little to cater for recurrent infrastructure related capital expenditure so the LHD must compete politically and make the case why their institutions are more deserving than others (that might be in more politically sensitive electoral seats). The Board has a responsibility to the community it serves to try and advocate for its’ cause. The CEO should support the actions of the Board but must also accommodate the bidding of the State and not cause embarrassment for it.
We must be recognize these issues but also manage them. The Board must not let the the CEO control its’ agenda. The Board must manage the performance of the CEO and be prepared to penalise him/or for failing in either management of the LHD budget or in advocacy for the LHD.
Information Service Denial (ISD)
Some of my blog posts are titled “Things they didn’t teach in medical school”.
Well I’m tempted to start another series entitled “Things my IT department won’t do for me”.
Years ago a colleague, A/Prof Matthew Links @cancersolutions tried to introduce the Moodle LMS for our oncology unit. It was blocked. No internal hosting and then no access to the external site through a firewall. Ironically – Moodle became the LMS of choice for our organisational learning unit and it is now accessible remotely.
Now we have two new problems – you can’t access any web-service (e.g. an online reference manager)that links to social networking. You can’t Facebook or tweet on hospital time……unless of course you own a mobile phone. Hmmm, I think the number of smartphones per person in our hospital is 1.2 so chances that there isn’t use of social media that is more disruptive than doing it from your hospital desktop are zilch.
The other problem is we can’t use Skype or similar services to support or clinical and educational activities. We have a registrar seconded to a satellite hospital which is 20 mins away by car. We can’t simply video-link them for a journal club. Skype or similar would be the simple solution. The alternatives – full Telstra-based video link or Webex and teleconferencing seem too hard and too expensive. And nobody want to help. Yet, if I were sitting in Tampa I could fly-by-wireless my drone into a bombing strike somewhere in Afghanistan.
It’s time the technology departments of the Australian public hospital system worked out what was happening in the outside world and caught up very quickly…..maybe in a Moore’s Law propotionality.
